Taste or smell?
We often think that we taste, but in fact we perceive smell. This also applies to wine. To unravel its secrets, you first need a good sense of smell. The nose is the most developed human sensory organ.
The smell of wine is transmitted by volatile substances. They make up most of its aroma. Chemically, volatile substances are associated with alcohol, aldehydes, esters, acids and other hydrocarbon compounds. The more hydrocarbon atoms they contain, the more intense the odor. The most intense odors come from esters. They have the highest volatility, even higher than aldehydes, which in turn smell stronger than alcohol. Acids have the least volatility.
Olfactory organ
The human olfactory zone is located in a small lateral chamber in the upper part of the nasal cavity. The air flow during inhalation does not enter this olfactory zone directly. First, the air must reach this side chamber, in which the olfactory sensations appear. The olfactory receptors themselves are located on the mucous membrane and occupy a space of no more than one square centimeter. The mucous membrane is covered with a moist film that dissolves odor molecules. The smell can only be perceived when wet. Nostrils with a moistened nasal septum, on the contrary, do not have an olfactory function. They are needed only to filter, draw in air, warm it and humidify it. Since the lateral chamber with the olfactory mucosa opens into the cavity of the tonsils, the olfactory receptors are more irritated when exhaling than when inhaling. This is the reason why you are often left with a long aftertaste as a result of swallowing wine.
Brain tissue
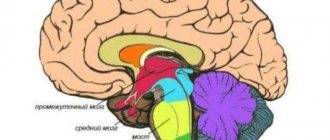
The structure of the human brain consists of the cerebral cortex, thalamus, cerebellum, brainstem and basal ganglia. The collection of nerve cells is called gray matter. Nerve fibers are white matter. The white color of the fibers comes from myelin. When the amount of white matter decreases, serious disorders such as multiple sclerosis occur.
The brain includes shells:
- The dura attaches to the skull and cerebral cortex.
- The soft tissue consists of loose tissue, is located on all hemispheres, and is responsible for saturation with blood and oxygen.
- The arachnoid is located between the first two and contains cerebrospinal fluid.
Liquor is located in the ventricles of the brain. When it is in excess, a person experiences headaches, nausea, and hydrocephalus occurs.
Olfactory neurons
On the olfactory mucosa of the nasal cavity there are about 50 million neurons in the form of small hairs “floating” in the mucosa. Neurons are the link between the nasal cavity and the brain. They transmit olfactory impulses from receptors to the centers of the brain responsible for smell. The path, as we see, is not long, and this is evidence that the human central nervous system is very closely connected with olfactory sensations. The olfactory centers of the brain decipher the information received and form a homogeneous olfactory impression, which is necessary since millions of neurons are stimulated simultaneously when they encounter odor molecules. Scientific research has shown that the human brain can recognize up to 4,000 odors. Smell memory is a very important factor when tasting wine. This is not an innate, but an acquired quality of a person that can be developed if there is a desire.
The area of the brain responsible for smell is capable of perceiving up to 4,000 different odors.
Medulla
It is located on the border of the spinal cord and the bridge and is responsible for vital functions.
The oblong part consists of elevations called pyramids. Its presence is characteristic only of erectus. Thanks to them, thinking appeared, the ability to understand commands, and small movements were formed. The pyramids are no more than 3 cm long; they are flanked by olive trees and posterior pillars. They have a large number of pathways throughout the body. In the neck region, motor neurons on the right side of the brain go to the left side and vice versa. Therefore, the loss of coordination occurs on the opposite side of the problem area of the brain.
The cough, respiratory and swallowing centers are concentrated in the medulla oblongata, and it becomes clear which part of the brain is responsible for breathing. When the ambient temperature drops, skin thermoreceptors send information to the medulla oblongata, which reduces the breathing rate and increases blood pressure. The medulla oblongata forms appetite and thirst.
Suppression of the function of the medulla oblongata may be incompatible with life. There is a violation of swallowing, breathing, and heart activity.
The medulla oblongata is a direct continuation of the spinal cord upward, which explains its name, and in front it passes into the hindbrain. Its rear end is narrow, and its anterior end is wide.
On the anterior and posterior surfaces of the medulla oblongata there is one longitudinal groove, which is a direct continuation of the same grooves of the spinal cord. On each side of the anterior groove there is one protrusion called a pyramid.
Structure of the medulla oblongata
If you dissect the medulla oblongata across, then on the cut surfaces you can see areas of gray matter (clusters of nerve cells), which are called olives, reticular formation (a diffuse cluster of cells of various types, which are densely intertwined with many fibers running in different directions.
Functions of the medulla oblongata: the reticular formation is also present in other parts of the brain and plays a large role in regulating the excitability and tone of all parts of the central nervous system, etc. They are related to the regulation of balance and coordination of body movements, metabolism, respiration, and blood circulation. Here are the centers of the reflexes of sucking, swallowing, coughing, sneezing, and blinking.
White matter consists of fibers through which nerve impulses travel from the hindbrain to the spinal cord and in the opposite direction.
It is a continuation of the spinal cord. The structure of the brain and spinal cord have much in common. This becomes clear upon a detailed examination of the white matter of the medulla oblongata. The white matter of the brain is represented by long and short nerve fibers. Gray matter is presented in the form of nuclei. This brain is responsible for coordination of movement, balance, regulation of metabolism, blood circulation and breathing. It is also responsible for coughing and sneezing.
The structure of the brain stem: it is a continuation of the spinal cord, divided into the midbrain and hindbrain. The trunk is called the medulla oblongata, midbrain, diencephalon and pons. The structure of the brain stem consists of ascending and descending pathways that connect it with the brain and spinal cord. It controls articulate speech, breathing and heartbeat.
Odor threshold
There is hardly any innate talent for tasting wine, although the area of the mucous membrane that perceives odors is not the same in all people. But still, the point is not in the number of receptors, but in their sensitivity. Some people respond to 100 odor molecules, others to 10,000. However, odor perception is thought to be largely regulated by the brain. This means that the ability to discriminate odors depends on knowledge of the components of the odor and on the willingness to distinguish them. Olfactory acuity can thus be developed, at least in relation to wine. There are also limitations. People who are surrounded by strong odors (tobacco, exhaust fumes) for a long time almost stop noticing them. They become insensitive to odors. With age, the acuity of smell also decreases. Whether this is due to the “wearing out” of the receptors or a weakening of concentration has not yet been clarified. It is known for sure that the acuity of smell decreases during the day in both young and elderly people. After breakfast, lunch and dinner it is especially low. On an empty stomach, on the contrary, a person “hears” smells very well.
Cerebellum and motor coordination disorder
Human motor skills are characterized by the accuracy of purposeful movements, which is ensured by the proportional work of many muscle groups, controlled voluntarily and automatically. This complex multifunctional system is implemented by a multineural coordinating apparatus that controls the balance of the body, stabilizes the center of gravity, regulates the tone and coordinated various activities of the muscles. The center of coordination of movements is the cerebellum; functionally, it contains the body of the cerebellum, consisting of two hemispheres, the vermis and three pairs of peduncles.
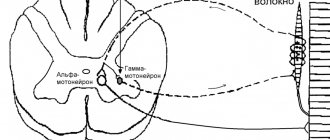
In the implementation of voluntary movement, the main role of the cerebellum is to coordinate the fast and slow components of the motor act. This becomes possible thanks to the bilateral connections of the cerebellum with the muscles and cerebral cortex. The cerebellum receives afferent impulses from all receptors irritated during movement (from proprioceptors, vestibular, visual, auditory, etc.). Receiving information about the state of the motor system, the cerebellum influences the red nucleus of the brain, which sends impulses to the γ-motoneurons of the spinal cord, which regulate muscle tone. In addition, part of the afferent impulses through the cerebellum enters the cerebral cortex of the motor zone (precentral and frontal gyri).
The main function of the cerebellum is carried out at a subconscious level. Efferent impulses from the cerebellar nuclei regulate proprioceptive stretch reflexes. During muscle contraction, the proprioceptor of the synergist muscles and antagonist muscles are excited. Normally, the transformation of voluntary movement into a complex reflex does not occur due to the inhibitory influence of cerebellar impulses. Therefore, when the cerebellum is damaged, disinhibition of segmental proprioceptive reflexes is manifested by movements of the limbs like ataxia.
The cerebellum has many afferent and efferent connections. Posterior spinocerebellar tract (Flexig's tract). The first neuron is located in the spinal ganglion; the axon in the dorsal root, through the dorsal horn, approaches the cells of Clark's column. The fibers of these second neurons are directed to the outer layers of the posterior part of the lateral funiculus on their side, ascend along the entire spinal cord and, at the level of the medulla oblongata, as part of the inferior cerebellar peduncle, enter the cerebellar vermis. This pathway is referred to as the posterior spinocerebellar tract. In the cortex of the cerebellar vermis there is a third neuron that contacts the piriform neurons of the cerebellar hemisphere cortex. The axons of the latter go to the dentate nucleus. The fibers of this fifth neuron are part of the superior cerebellar peduncle. The right and left superior cerebellar peduncles cross - Wernicke's cross - and end at the red nucleus cells of the opposite side. The axons of the cells of the red nucleus are immediately directed to the opposite side of the midbrain and form a ventral decussation in the tegmentum of the midbrain - the decussation of Forel, pass as part of the lateral cord of the spinal cord, and reach the cells of the anterior horns. The set of axons of the cells of the red nucleus is called the Monakov bundle.
Govers' anterior spinocerebellar tract. The first neuron is located in the spinal ganglion, the second neuron is a cell of the dorsal horn, but its axons move to the opposite side and go up the spinal cord, in the anterior part of the lateral cord, pass through the medulla oblongata, the pons of the brain, at the level of the superior medullary velum they pass to the opposite side side and as part of the superior cerebellar peduncle reach the cells of the cerebellar nuclei.
The cerebellum receives afferent proprioceptive impulses not only along the Flexig and Gowers pathways, they also arrive along the axons of the cells of the nuclei of the thin and cuneate fasciculi, some of which go through the lower cerebellar peduncles to its vermis.
In addition, the axons of the cells of the vestibular nuclei go to the cerebellum as part of the inferior peduncle - mainly from the vestibular lateral nucleus of Deiters, they end in the nucleus of the cerebellar clivus. The fibers of the cells of this nucleus, as part of the upper and, possibly, lower cerebellar peduncles, approach the cells of the reticular formation of the brain stem and the vestibular lateral nucleus, from which the conductors form the descending tracts - vestibulospinal and reticular-spinal, ending at the cells of the anterior horns of the spinal cord. This pathway regulates the balance of the body.
From the cerebellum, through the vestibular lateral nucleus, connections are established with the nuclei of the oculomotor nerves (as part of the medial longitudinal fasciculus).
The cerebellum has numerous connections with almost all lobes of the brain. There are 2 massive beams.
The fronto-pontine-cerebellar is a collection of axons of cells predominantly in the anterior sections of the superior and middle frontal gyri. In the depths of the lobe, they are collected in a compact bundle and form the anterior leg of the internal capsule. Then the cerebral peduncles pass through the base and end with a synapse at the cells of the pons. The axons of the second neurons move to the opposite side of the pons and, as part of the middle cerebellar peduncle, enter its hemisphere, contacting the cells of the cerebellar cortex. The processes of these neurons approach the dentate nucleus. The fibers of the dentate nucleus cells in the superior cerebellar peduncle reach the red nucleus of the opposite side and carry impulses along the reticular-spinal tract that regulate human posture in an upright position, in particular standing and walking.
Occipitotemporal ponsocerebellar tract - its first neurons are located in the cortex of the occipital and temporal lobes; their axons gather in the subcortical white matter, then, as part of the posterior femur of the internal capsule, they go at the base of the midbrain to the pons nuclei of their side. The axons of the pontine cells move to the opposite side and reach the cerebellar cortex along the middle peduncle. The fibers of these cells approach the dentate nucleus, which has connections with the brain stem. With the help of these tracts, coordination of the cerebellum with the organs of vision and hearing is ensured.
Ultimately, the existing decussations of the cerebellar afferent and efferent systems lead to homolateral communication of one hemisphere of the cerebellum and the limbs. When the cerebellar hemisphere is damaged, disorders of its function occur on the same half of the body. Lesions in the lateral funiculus of the spinal cord also cause cerebellar disorders on its half of the body. The cerebral hemispheres are connected to the opposite hemispheres of the cerebellum. Therefore, when the cerebral hemispheres or the red nucleus are damaged, cerebellar disorders are detected on the opposite side.
THE CONCEPT OF ATAXIA, TYPES OF ATAXIA
Ataxia is a form of erratic movement, taxis - from the Greek. order, a- negation. It occurs when there is a violation of the coordination of the action of muscle groups - agonists (directly carrying out the movement), antagonists (in some phase counteracting the agonists), synergists (helping the work of either agonists or antagonists). Movements lose coherence, accuracy, smoothness, proportionality and often do not achieve the goal. Such a patient's muscle strength remains sufficient, he has sufficient strength, he has no paresis.
The pathogenetic essence of ataxia consists of:
1. Violation of reciprocal innervation. The mechanism of reciprocal (coupled) inhibition of spinal motor centers is as follows: the axons of receptor cells (in the spinal ganglia) in the spinal cord are divided into branches, some of them excite motor neurons of the flexor muscles, and others contact with intercalary cells, which have an inhibitory effect on extensor muscle cells. The complex integrative function of this mechanism also involves cerebellar impulses.
2. Termination of proprioceptive signaling (from muscle spindles, Golgi tendon bodies) along one or another ascending afferent pathway. Information about the degree of muscle tension at any given moment and about the results of the adaptive effects of functional systems ceases to be received. The side of the motor function that is referred to as reverse afferentation is upset.
Types of ataxia.
1. Sensitive ataxia is associated with simultaneous suffering in coordination of movements and muscle-articular sensation. With severe ataxia in the upper limb, it is difficult to perform the simplest actions. At rest, involuntary movements are sometimes observed in the fingers of the hand, reminiscent of athetosis - pseudoathetosis. Coordination of movements is also impaired in the lower extremities, which is confirmed by missed hits and jerking movements when performing the heel-knee test. Muscle tone in the affected limbs is reduced in both the flexor and extensor muscles. In a standing position, staggering is noted, especially when performing the Romberg test. Movement becomes uncertain, the patient walks with his head down, controlling the act of walking with the help of vision. Thus, sensitive ataxia is always combined with a disorder of deep sensitivity and functional separation of individual segments of the limbs from the higher areas of the brain. Another characteristic feature of this type of ataxia is that it intensifies when the control of the visual analyzer is turned off. Sensitive ataxia with damage to the posterior cords of the lower half of the spinal cord (for example, with syphilis, funicular myelosis - B12) may be accompanied by the disappearance of deep reflexes in the lower extremities, which is explained by degeneration of the collaterals of the thin bundle fibers, which are the afferent part of the deep reflex arc.
2. Cerebellar ataxia. Associated with damage to the cerebellar systems. Considering that the cerebellar vermis takes part in the regulation of contraction of the muscles of the trunk, and the cerebral cortex of the distal limbs, two forms of cerebellar ataxia are distinguished.
- Static-locomtor - when the cerebellar vermis is damaged, mainly standing and walking are disrupted. The patient stands with his legs wide apart and sways. When walking, the body deviates to the sides, the gait resembles the gait of a drunk. Turning is especially difficult. Deviations when walking are observed towards the cerebellar lesion. Stability is tested in the Romberg position. If the cerebellar structures are damaged, the patient in this position sways in the appropriate direction; with staggering in the anteroposterior direction - characteristic of damage to the anterior parts of the cerebellar vermis. The patient's walking in a straight line is examined, as well as the flank gait—stepping movements to the side. At the same time, pay attention to the clarity of the step and the ability to quickly stop in case of a sudden command. When the cerebellar structures are damaged, the combination of simple movements that make up a sequential chain of complex motor acts is disrupted. This is referred to as asynergy and is determined using the Babinski test.
- Dynamic ataxia - with it, the performance of various voluntary movements of the limbs is impaired. This type of ataxia mainly depends on damage to the cerebellar hemispheres. This is detected when studying the movements of the upper extremities, for example, when performing the finger-to-toe, heel-knee, test for diadochokinesis, etc.
In addition to disruption of these tests with movements of the limbs, when the cerebellum is damaged, speech is disrupted - as a result of incoordination of the speech motor muscles, speech loses smoothness, becomes explosive, stress is placed on the wrong syllables - scanning speech; The handwriting changes - the handwriting becomes uneven, large - megalography. Nystagmus is observed - a rhythmic twitching of the eyeballs when looking to the sides or up - a kind of intention tremor of the oculomotor muscles. When the cerebellar structures are damaged, the plane of nystagmus coincides with the direction of voluntary movements of the eyeballs - when looking to the side, the nystagmus is horizontal, when looking up and down - vertical. Sometimes nystagmus is congenital. Such nystagmus is usually present not only when the eyeballs are abducted to the sides (with tension), but also when looking straight (“spontaneous nystagmus”).
When the cerebellar systems are damaged, muscle tone may change. The most common symptom is muscle hypotonia: the muscles become flabby, flaccid, and joint hypermobility is possible. This may reduce deep reflexes.
Coordination of movements is impaired when the frontal and temporal lobes and their conductors are damaged. In this case, walking and standing are disrupted, the torso deviates posteriorly and in the direction opposite to the lesion. Missing in the arm and leg (hemiataxia) is detected. With this type of coordination disorder, other signs of damage to the corresponding lobes of the cerebral hemispheres are also found.
3. Cortical ataxia. Coordination of movements is impaired when the frontal and temporal lobes and their conductors are damaged. In this case, walking and standing are disrupted, the torso deviates posteriorly and in the direction opposite to the lesion. Missing in the arm and leg (hemiataxia) is detected. With this type of coordination disorder, other signs of damage to the corresponding lobes of the cerebral hemispheres are also found.
4. Vestibular ataxia - occurs when the function of the vestibular analyzer, in particular its proprioceptors in the labyrinth, is impaired. With it, the balance of the body is upset; while walking, the patient deviates towards the affected labyrinth. Systemic dizziness, nausea, and horizontal rotatory nystagmus are characteristic. Hearing may be impaired on the side of the affected labyrinth.
Thus, a disorder of coordination of voluntary movements is observed with damage to both the cerebellum itself and the conductors through which impulses from the muscles, semicircular canals of the inner ear and cerebral cortex are brought to it and taken away from the cerebellum to the motor neurons of the brain stem and spinal cord. Patients with damage to the cerebellar systems usually do not show any pathological manifestations at rest. Various types of incoordination appear in them only when muscles are tense.
Functions of departments
The forebrain includes the most recently developed parts. And this means that it is thanks to them that a person has the qualities that he has. And if the diencephalon is mainly concerned with the regulation of metabolism, primitive reflexes and needs, as well as simple motor activity, then the hemispheres are the very place where conscious thoughts arise, where learning and memorization of information occurs, and something new is created.
The hemispheres are also conventionally divided into several parts-zones: parietal, frontal, posterior and temporal. And here there are cells that are involved, among other things, in the analysis of information coming from outside: visual, auditory, olfactory, gustatory and tactile centers.
The most interesting thing is that from a functional point of view, the left and right hemispheres are different. Of course, there are cases when, when one part of the brain was damaged, another took over its tasks, that is, there is a certain interchangeability, but in a normal case the situation could be like this: the left hemisphere is engaged in analyzing the intonation of another person’s speech, and the right hemisphere is engaged in interpreting the meaning of what was said. This is why left-handers and right-handers, who have more developed different parts, think slightly differently.
Also, the functions of the forebrain include memory, various reactions to external stimuli, planning and constructing future scenarios and situations. The speech center is also located here. All higher nervous activity takes place here: creativity, reflection, ideas.
It is also quite interesting that the forebrain actively develops not only in the prenatal period, but also in the first few years of life. Every new skill and skill, a learned word, any important information - all this forms new neural connections. And this kind of map is unique for each person.
intermediate;
average;
oblong.
cerebral hemispheres;
brain stem;
cerebellum.
Signs of poor coordination
Loss of stability is classified according to the phases of movement and the expected diagnosis. Slow action, unstable body position are a common symptom of polyneuritis.
Involuntary twitching (chorea) is a consequence of damage to the central nervous system after rheumatism or a symptom. Chaotic muscle contractions indicate a latent form of epilepsy. If the gait is unbalanced, the cerebellum and cerebral circulation are examined.
Symptoms of impaired motor coordination:
- profuse sweating;
- blood pressure surges;
- changes in breathing rhythm, skin color of the face and neck;
- movement coordination disorder;
- sudden attacks of nausea.
The altered state is accompanied by involuntary movements of the eyeball (nystagmus): vertical, rotary, transverse, diagonal. There is paroxysmal positional with the formation of the illusion of rotation of the external picture. Ringing in the ear signals problems with receptors in the peripheral region.