Functions of the Sylvian aqueduct
The Sylvian aqueduct, connecting the ventricles, ensures the trophic function of these structures. Incoming nutrients form the proper functioning of brain cells. The aqueduct of Sylvius circulates cerebrospinal fluid (CSF) and creates pressure. Liquor is a colorless liquid that is located in the ventricles of the brain in the subarachnoid space.
Liquor will keep the brain and spinal cord suspended, providing its protection and creating conditions for its vital functions. Cerebrospinal fluid also participates in metabolic processes, delivering oxygen and nutrients from the bloodstream to nerve cells. Hormones are produced and processes in the body are regulated by the brain.
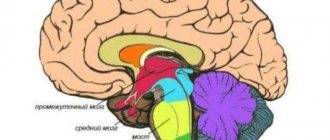
Midbrain
Very often questions arise about the brain. A table of its structural elements helps explain their functionality.
| Divisions of the brain | Functions |
| Medulla | Regulates heart rhythm, breathing, blood pressure |
| Bridge | Responsible for eye movement and facial expressions |
| Midbrain | Reflex movement of the head |
| Diencephalon | Controlling the functioning of internal organs |
| Cerebellum | Responsible for clear coordination |
It is the midbrain that is responsible for visual and auditory reflexes. And its central part regulates unconscious stereotypical movements: tilts and turns of the head and torso.
In terms of complexity, the midbrain is inferior to other parts of the brain. That's why it is studied the least.
The parts of the midbrain are the roof, the tire, and the legs. Inside there is a narrow channel called the cerebral aqueduct. It is designed to connect the ventricles of the diencephalon and rhombencephalon.
The midbrain is responsible in the human body for orientation reflexes, postures, vision, hearing, chewing and swallowing movements, and muscle tone.
Types of pathologies and clinical symptoms
The Sylvian aqueduct performs important functions, so pathological processes lead to disruption of the brain.
The most common causes of dysfunction of the aqueduct are narrowing (stenosis), obstruction of the lumen by a tumor, and congenital anomalies of the development of the aqueduct.
The most common disease caused by changes in the structure of the canal is hydrocephalus.
Hydrocephalus is the accumulation of cerebrospinal fluid in the cavities (ventricles) of the brain. It can develop in both children and adults.
In childhood, it develops in newborns.
The cause of cerebral hydrocele is anomalies in the development of the Sylvian aqueduct, provoked by severe stress, bad habits, infectious processes in the mother, birth trauma and non-compliance with doctor’s recommendations.
It is easy to detect brain hydrocephalus in a baby: the head is enlarged in size, he is restless (cries constantly). The forehead increases in size, veins bulge in the frontal and temporal areas, it grows slowly and slowly gains weight, develops slowly (begins to sit by 10 months, crawl by 12 months), and cannot smile. There is a characteristic divergent squint, deep-set eyes due to the overhang of the forehead, etc. By the age of one year, babies begin to experience convulsions.
In children over 2 years of age, the causes of hydrocephalus are head injuries and tumors. The clinical picture is different. Children are bothered by headaches accompanied by nosebleeds, pressing pain in the eye area, restless sleep, and lack of coordination due to damage to the cerebellum. They are hyperactive, irritable (they want more attention). They also cannot control the act of urination, during which a large amount of urine is released (polyuria). Over time, they lose vision, they develop bluish circles before their eyes, obesity, and convulsions.
In adults, hydrocephalus develops as a complication of other diseases.
After a stroke, traumatic brain injury, tumors, degenerative changes in dementia and encephalopathy, the likelihood of developing cerebral hydrocele is very high.
It can be detected by the following symptoms:
- headaches that appear after sleep (caused by compression in the foramen magnum and increased intracranial pressure;
- dyspeptic disorders (nausea, vomiting in the morning);
- drowsiness;
- depression of consciousness from stupor to coma caused by compression of the medulla oblongata;
- dysfunction of the oculomotor muscles;
- congestion in the optic nerve head, causing decreased visual acuity.
Hydrocephalus against the background of dementia (dementia) develops within 20-30 days and is manifested by apathy to everything that happens, decreased memory (does not remember your age), and confuses daytime with nighttime.
Apraxia also occurs; a person lying down can simulate walking, but in a standing position he cannot do this. Hydrocephalus in dementia differs in that there are no problems with urination and vision.
Causes
Three pathological mechanisms lead to the accumulation of an excess amount of cerebrospinal fluid in the cerebrospinal fluid system of the brain: the production of an excess amount of cerebrospinal fluid, a violation of its absorption, or a disorder of the cerebrospinal fluid circulation. Hydrocephalus may be based on one of these mechanisms or a combination of them. The causes that cause disturbances in the functioning of the cerebrospinal fluid system can act during fetal development and cause congenital hydrocephalus or affect the brain after birth and cause the appearance of so-called acquired hydrocephalus.
The causes of congenital hydrocephalus include malformations of the cerebrospinal fluid system (atresia of the foramina of Magendie and Luschka, defects in the structure of the subarachnoid space, stenosis of the Sylvian aqueduct, Dandy-Walker syndrome, etc.), craniovertebral anomalies (Chiari malformation, congenital basilar impression), intrauterine infections (toxoplasmosis , congenital syphilis, cytomegaly, rubella), birth trauma.
Acquired hydrocephalus can occur as a result of inflammatory processes in the brain and its membranes (encephalitis, arachnoiditis, meningitis), traumatic brain injury, vascular disorders (bleeding into the ventricles, hemorrhagic stroke or intracerebral hematoma with blood breaking into the ventricles). Hydrocephalus often develops against the background of a colloid cyst of the third ventricle and intracerebral tumors (astrocytomas, germinomas, ganglioneuromas, etc.), which grow into the ventricles of the brain or compress the cerebrospinal fluid pathways, thereby disrupting the normal circulation of cerebrospinal fluid and its outflow from the cranial cavity.
Separately, there is an atrophic (replacement) form of hydrocephalus, which occurs as a result of post-traumatic death or age-related atrophy of brain tissue. In this case, cerebrospinal fluid fills the space that is formed inside the skull as a result of a decrease in the volume of the brain. Atrophic hydrocephalus in old age can develop against the background of impaired blood supply to the brain due to atherosclerosis of cerebral vessels, hypertension, and diabetic macroangiopathy.
Diagnosis of the disease
When the first symptoms appear, you should immediately consult a neurologist. After collecting complaints and asking about the possible causes of the pathology, instrumental research methods will be prescribed.
Computed tomography is used to determine normal/pathological processes in brain structures. With its help, benign and malignant neoplasms, changes in the contours of the ventricles and subarachnoid space are identified.
MRI is used to determine the type of hydrocephalus.
Cisternography is performed to determine the direction of the flow of cerebrospinal fluid and the location of its accumulation.
Angiography of cerebral vessels - the presence of occlusion in the arteries.
Pathogenesis
Normally, cerebrospinal fluid (CSF) is produced by the choroid plexus of interconnected ventricles of the brain. The largest amount of it is formed in the lateral ventricles, from where the cerebrospinal fluid enters the third ventricle, and from it through the Sylvian aqueduct into the fourth ventricle. Then the cerebrospinal fluid enters the subarachnoid (subarachnoid) space, which extends over the entire surface of the brain, and in the caudal direction passes the region of the craniovertebral junction and then surrounds the spinal cord along its entire length. The cerebrospinal fluid located in the subarachnoid space is constantly absorbed by the arachnoid (arachnoid) membrane of the spinal cord and brain and enters the blood. The above etiological factors that disrupt the production, movement and absorption of cerebrospinal fluid lead to its excessive accumulation and the occurrence of hydrocephalus.
Treatment methods
Treatment of pathology of the cerebral aqueduct is based on eliminating the underlying disease that led to the development of stenosis or occlusion.
Conservative treatment is used to eliminate clinical symptoms. Non-steroidal anti-inflammatory drugs (ketolac, ketanov, nimesil) are effective in combating pain.
To combat edematous syndrome, diuretic drugs (furosemide, veroshpiron, mannitol) are used.
In order to dilate blood vessels, vasoactive substances are needed, which also prevent the development of cerebral edema (magnesium sulfate).
To ensure restful sleep - phenobarbital.
The most effective is complex treatment, combining conservative and surgical measures.
For better outflow of cerebrospinal fluid in the area of the brain canal and ventricles, additional openings are surgically created. Then a bypass is performed (connection to the right atrium, abdominal cavity, etc.) in order to get rid of the accumulation of cerebrospinal fluid in the cavities of the brain.
If there is a tumor in the area of the Sylvian aqueduct, it is removed surgically.
Classification
According to the etiological principle, congenital and acquired hydrocephalus are distinguished.
According to the mechanism of occurrence, hydrocephalus is classified into open and closed forms. Open hydrocephalus is associated with overproduction of cerebrospinal fluid or impaired absorption during normal cerebrospinal fluid circulation. Closed hydrocephalus is caused by a violation of the outflow of cerebrospinal fluid due to compression, partial or complete obstruction of any part of the cerebrospinal fluid system of the brain.
Depending on where the excess accumulation of cerebrospinal fluid occurs, internal and external hydrocephalus are distinguished. Internal hydrocephalus is accompanied by the accumulation of cerebrospinal fluid in the ventricles of the brain. External hydrocephalus is characterized by excess cerebrospinal fluid in the subarachnoid and subdural space.
According to the characteristics of its course, hydrocephalus is classified as acute, subacute and chronic. Acute hydrocephalus is characterized by rapid development, in which decompensation occurs a few days after the onset of the first signs of the disease. Subacute hydrocephalus develops within a month, and chronic hydrocephalus develops over six months.
Of great clinical importance is the division of hydrocephalus into stabilized (compensated) and progressive (increasing). Stabilized hydrocephalus does not grow and usually occurs with normal cerebrospinal fluid pressure. Progressive hydrocephalus is characterized by worsening symptoms, is accompanied by an increase in cerebrospinal fluid pressure, does not respond well to conservative therapy and leads to atrophy of brain tissue.
2. Main locations of meningiomas
Meningiomas “prefer” areas of the brain where the arachnoid meninges are well developed. In most cases, these neoplasms are localized on the convexital surface of the brain (in the frontal, parietal and occipital regions), in the area of the parasagittal sinus/falx, pyramids of the temporal bone, in the cavernous sinus, olfactory fossa, Sylvian fissure, optic nerve canal, etc. Much less often, these tumors are present in the cavities of the ventricles or on bone tissue. Depending on the location, meningiomas are divided as follows:
- convexital;
- parasagittal;
- basal.
Sources
- https://mozgius.ru/stroenie/silviev-vodoprovod.html
- https://glmozg.ru/bolezni/kisty/arahnoidalnaya-kista-golovnogo-mozga.html
- https://www.krasotaimedicina.ru/diseases/zabolevanija_neurology/hydrocephalus
- https://NeuroDoc.ru/anatomy/silviev-vodoprovod.html
- https://fb.ru/article/290268/silviev-vodoprovod-stroenie-i-funktsii
- https://medintercom.ru/articles/meningioma_silvievoy_sheli
[collapse]
3. Symptoms of Sylvian fissure meningioma
The Sylvian fissure (sulcus) separates the temporal and frontoparietal lobes of the brain. This groove is one of the deepest in the brain; it runs along the lateral periphery of the hemisphere from top to bottom/anterior, dividing into three branches.
Meningioma of the Sylvian fissure has symptoms that are characteristic of almost most tumors of the frontal lobe of the brain:
- mental disorders (emotional instability, primitive behavior);
- personal changes;
- epileptic seizures;
- Broca's aphasia (speech disturbances/difficulties);
- impaired coordination of movements;
- olfactory disturbances;
- hyperkinesia (uncontrolled movements);
- convulsions.