Syndromes involving the pyramidal tract and extrapyramidal system
Our brain is a unique multi-complex system that simultaneously controls the sensory and vestibular apparatus, movement, thinking, speech, vision and much more.
In this article we will talk about how the brain controls voluntary and involuntary movement. And about what neurological abnormalities are associated with damage to the pyramidal system of the brain.
Pyramidal and extrapyramidal tract
The pyramidal system consists of pyramidal and extrapyramidal tracts. What is their difference? The pyramidal tract, or tractus pyramidalis, is a pathway that connects cortical neurons responsible for motor activity with the nuclei of the spinal cord and cranial nerves.
Its job is to control voluntary muscle movements by transmitting signals from the central nervous system to the body. But the extrapyramidal one, it controls the unconscious conditioned reflexes of our body. This is an older and deeper structure of the brain, and its signals are not reflected in consciousness.
Extrapyramidal and pyramidal are descending pathways. And the ascending main pathways are responsible for transmitting information from the senses to the brain. These include: the lateral spinothalamic tract, the anterior spinocerebellar tract and the posterior spinocerebellar tract.
Pyramidal tracts of the brain. Structure
They are divided into 2 types: corticospinal and corticonuclear. The corticospinal cord is responsible for the movements of the torso, the cortico-nuclear cord controls the facial and swallowing muscles.
How does the corticospinal pyramidal tract work? This electrical path begins from the cerebral cortex - the area that is responsible for higher mental activity, for consciousness. The entire cortex is made up of interconnected neural networks. More than 14 billion neurons are concentrated in the cortex.
In the hemispheres, information is redistributed in this way: everything that concerns the work of the lower extremities is located in the upper sections, and everything that concerns the upper, on the contrary, is in the lower structures.
All signals from the upper and lower parts of the cortex are collected and transmitted to the internal capsule. Then, through the midbrain and through the middle part of the pons, a bundle of nerve fibers enters the pyramids of the medulla oblongata.
Here branching occurs: most of the fibers (80%) pass to the other side of the body and form the lateral spinal tract. These branches “launch” motor neurons, which then transmit signals to contract or relax directly to the muscles. A smaller part of the fiber bundle (20%) innervates the motor neurons of “their” side.
The corticonuclear pyramidal tract initially passes through the same brain structures as its “partner”, but crosses over in the midbrain and goes to the facial neurons.
Anatomical features important for diagnosis
The pyramidal pathway has some structural features that should not be overlooked when it is necessary to determine the localization of the pathology. What specific features do you need to know?
- Some of the nerve fibers of the corticospinal tract, in addition to the lateral decussation, also intersect in the area of the white commissure of the spinal cord segment, where they end.
- Most of the muscles in the trunk are controlled by both hemispheres of the brain. This is an important protection. In the event of a stroke or stroke, those patients diagnosed with hemiplegia can support the body upright.
- In the area of the pons, the fibers of the corticospinal tract are separated by other fibers - the cerebellar tract. Divided bundles emerge from the bridge. In this regard, movement disorders are often dispersed. Whereas the pathological focus may be single.
Symptoms of damage to the pyramidal tract are sometimes quite obvious, as in the case of paraplegia, for example. But sometimes it is difficult to determine the cause. It is important to notice minor disturbances in motor skills in time and see a doctor.
Symptoms of defeat. Levels
Clinical manifestations of pyramidal tract disorders depend on the specific part of the nerve fibers damaged. There are several levels of damage to motor activity: from complete paralysis to relatively favorable impairments.
So, neurology identifies the following levels of damage to the pyramidal tract:
- Central monoparesis (paralysis). The disorders are localized in the cerebral cortex (left or right).
- Central hemiparesis. The internal capsule is damaged.
- Various alternating syndromes - the brain stem area is affected.
- Paralysis of limbs. One of the lateral cords in the spinal cord.
Central paralysis with damage to the brain capsule and cerebral hemispheres is characterized by the fact that muscle function is impaired on the opposite side of the body relative to the affected area.
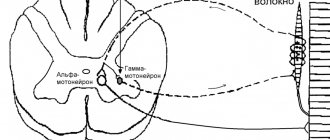
After all, the intersection of the pyramidal tract works in the nervous system. That is, the fibers move to the lateral or lateral spinal tract.
The simplified diagram shows how the pyramidal path, the anatomy of which was discussed above, crosses and moves on.
If the lateral cord in the spinal cord is damaged, the work of the muscles on the same side as the injury is disrupted.
Neuropathology. Peripheral and central paralysis
Nerve fibers look like cords under a microscope. Their work is extremely important for the body. If conduction in some part of the nerve chain is disrupted, muscles in some parts of the body will not be able to receive signals. This will cause paralysis. Paralysis is divided into 2 types: central and peripheral.
Source: https://eltransteh.ru/sindromy-porazhenija-piramidnogo-puti-i-jekstrapiramidnoj-sistemy/
Structure
The pyramidal system consists of a pyramidal tract formed by corticonuclear and corticospinal fibers. They are axons of neurons in the inner cortical layer of the telencephalon. They are localized in the precentral ridge (gyrus) and in the cortex of the parietal and frontal lobes. The primary motor field is located in the precentral crest along with pyramidal motor neurons, which are capable of controlling skeletal muscles as a whole (groups) or individually (1 muscle). Nerve cells that excite the lingual, pharyngeal and head muscles are localized in the lower parts of the ridge. Higher up, in the middle section, is the muscular system of the upper limbs and torso. The uppermost section provides nerve fibers to the muscle groups of the lower extremities.
Beginning of the pyramidal path (Kora)
The pyramidal system is the basis for the implementation of voluntary movements, starting in the 5th layer of the cerebral cortex, in the Betz motor cells.
The pyramidal tract is formed by myelin fibers passing through the white matter of the cerebral hemisphere and heading to the internal capsule. The knee of the capsule is formed by corticonuclear fibers, and the posterior limb of the internal capsule is partially formed by corticospinal fibers.
Pyramid Path
The fibers of the pyramidal tract first go to the basal part of the brain and then to the pontine region. They go through the front first. Then, passing through the brain stem, the corticonuclear fibers cross (transition to the opposite side) to the efferent nuclei of the oculomotor (III pair), trochlear (IV), trigeminal (V), abducens (VI), glossopharyngeal (IX), vagus ( X), accessory (XI) and hypoglossal (XII) nerves. The exception is the facial nerve (VII pair). Nerve fibers make the transition to the opposite side at the level of the nucleus, in the upper third. Partial fibers of the pyramidal tract from the brain stem are directed to the cerebellum.
Transition to the spinal cord
In the region of the medulla oblongata, the pyramidal tract passes through the pyramidal cells. At the junction of the pyramids and the spinal cord, the nerve bundles intersect. This cross divides the fibers into 2 unequal parts.
Division of the tract into the corticonuclear and corticospinal pyramidal tracts
80% of the nerve fibers go to the opposite side, forming the pyramidal lateral corticospinal tract in the lateral cord of the spinal cord. Fibers that do not cross into the anterior cord of the spinal cord, forming in it the anterior corticospinal tract. In the area of the white commissure, the fibers intersect. Many nerve fibers of the pyramidal tract terminate on interneurons of the anterior horns. They give rise to the development of the efferent components of the spinal nerves.
Localization (area of segments) Number of ending nerve fibers (cervical 50, thoracic 25%, lumbar 25%)
At the level of thoracic segments 3-5, the anterior corticospinal tract ends. Due to the crossing of nerve bundles in the pyramidal system, the left hemisphere of the brain is responsible for the innervation of the right half of the human body, and the right hemisphere is responsible for the innervation of the left half of the human body.
The corticonuclear pathway is associated with almost all nuclei of the cranial nerve. The exceptions are the purely sensory nerves olfactory, optic and vestibulocochlear nerves. Divided bundles of fibers also pass through the internal capsule in the white matter. Having reached the cranial nerve, the impulse is sent through separate bundles to the skeletal muscles. The corticonuclear tract controls facial expressions and swallowing muscles, while the corticospinal tract controls body and leg movements.
The pyramidal system is inextricably linked with the extrapyramidal system. They differ from each other in composition and functions.
The main differences of the extrapyramidal system are:
- it includes the basal ganglia, substantia nigra, red nucleus and other structures.
- performing complex unconscious motor acts: chewing food, playing sports (running);
- ensuring facial expressions;
- articulation of speech;
- ensuring muscle tone and its redirection during movements (posing and changing positions).
Pyramidal pathways (system) - description and functions
Neurology is the most precise science in medicine. This is what topical diagnostics does.
Topical diagnostics allows a neurologist, with the help of a hammer, questioning and examination, as well as when performing samples and tests, in some cases to localize the lesion located in the head or spinal cord with an accuracy of a millimeter. But earlier this science was applied, and even earlier it was descriptive, like all anatomy.
As a result, such names as “cerebellar peduncles”, “putamen”, “fence”, “tubercles of the quadrigeminal tuberosity”, “aqueduct” passing deep into the brain, and many other formations appeared.
Their functions were completely unknown for a long time. Scientists understood that the brain and spinal cord consisted of gray and white matter, but this was perhaps the only difference.
The internal structure was not amenable to analysis.
Dyes have not yet been invented that would make it possible to accurately show neurons and prove that the central nervous system consists of cells with the longest processes (sometimes up to a meter in length). The science of neuroanatomy was not invented.
And only after the advent of Virchow’s cellular theory, which placed the function of an organ in direct dependence on its cellular composition, after the advent of physiology, which studied the functions of neurons and how they differ, did an understanding of the integral work of a nerve cell arise.
The subsequent steps were taken by Sechenov and Pavlov.
An excellent illustration of this “internal formation” is the pyramid system. It is the main effector: with its help all motor conscious acts are performed.
If the pyramidal system were absent, then we would be immobile animals, like sponges or bryozoans, and all civilization would be impossible.
They usually say that civilization was created by the human brain and his hands, but they forget to say that the pyramidal path is precisely the intermediary that brings brain impulses for movement to the muscles.
What are the functions of a pyramid system? What is the diagram of the pyramid paths? We'll tell you about this .
What it is?
Pyramidal tracts (or system) are the second name for the corticospinal, efferent, or descending tracts. These pathways begin in the precentral gyrus, in its gray matter.
It is there that the bodies of neurons are located, which generate impulses for commands to the striated, or skeletal muscles.
These impulses are conscious, the pyramidal system obeys our will.
The pyramidal and extrapyramidal systems (unconscious) are combined into a single system of movement, coordination of balance and muscle tone.
The pyramidal tracts end in the anterior horns of the spinal cord, at its various levels - from the neck to the sacrum.
It is there that the switch occurs to large motor neurons, which directly terminate at the neuromuscular junction, in which the neurotransmitter acetylcholine gives the signal for muscle contraction.
This definition is a little vague, but it explains the essence. Let us consider in detail the anatomy and organization of the corticospinal tract and its structures at different levels.
Bark
Pyramidal tracts begin in the precentral gyrus, or more precisely, in its special field, which is projected along it in a narrow strip, from bottom to top. This band is called cytoarchitectonic field No. 4 according to Brodmann (yes, the cerebral cortex, like the earth’s crust, has its own architecture and architectonics).
In this field there are giant (they are indeed very large) pyramidal Betz cells (in memory of the Russian histologist and anatomist Vladimir Betz, who discovered these cells in 1874). Their task is to generate impulses for precise and targeted movements.
https://www.youtube.com/watch?v=YVIcFGF5AWw
In the lower sections there are neurons responsible for the movement of the pharynx and phonation, then, higher, there are cells that innervate the facial muscles, arms, then the torso and legs.
If you type the name “motor homunculus” into a search engine, you will see a picture of how the relative “powers” of this cortical zone are distributed among themselves.
A huge part of the nerve cells are responsible for fine movements of the hands and fingers, as well as for facial and vocal muscles.
But the innervation of the legs, which produce a small number of stereotypical movements, requires a small number of cells.
Cortical impulses generated by large Betz cells (for example, you are planning to move your finger) must reach the muscle as quickly as possible. After all, this is not the autonomic nervous system, which “slowly manages” inside the body. For example, the extraction of food depends on the quality and speed of voluntary movements.
Therefore, the axons of these neurons are well isolated, “of the highest class.” Their fibers have a thick, myelin sheath. This is the “elite” among all pathways; they include only 3-4% of axons from the total volume of the pyramidal system.
The remaining sources of impulses are smaller neurons located in other layers of the cortex.
In addition to the Brodmann area, there are also premotor areas that give off their impulses; they are also classified as the corticospinal tract.
It must be remembered that all the cortical structures we have mentioned perform movements on the opposite side of the body. Left neurons generate movements on the right, and vice versa.
The fact is that almost 90% of the total volume of fibers crosses below and moves to the other half of the body. What happens next?
The first “fork” and the corticonuclear pathway
Everyone knows that in addition to the muscles on the arms, legs and torso, there are also muscles on the face and head. Even before passing through the inner capsule (see below), the bundles are separated.
Therefore, the first, larger, bundle leaves the cortex to innervate the limbs and torso, and the second, smaller one, goes to the motor nuclei of the cranial nerves, which are also parts of voluntary and conscious movement.
The first remains the pyramidal fasciculus, and the second is called the corticonuclear, or corticonuclear tract . These nerves that “receive pyramidal nutrition” include:
- Oculomotor nerve (3 pairs) – movements of the eyes and eyelids;
- Trochlear nerve (4 pairs) – eye movements;
- Trigeminal nerve (5th pair) – chewing muscles;
- Abducens nerve (6th pair) – eye movement;
- Facial nerve (7th pair) – facial expressions;
- Glossopharyngeal nerve (9th pair) – stylopharyngeal muscle, pharyngeal constrictors;
- Vagus nerve (10th pair) – muscles of the pharynx, larynx;
- Accessory nerve (11th pair) – trapezius and sternocleidomastoid muscles;
- Hypoglossal nerve (12th pair) – muscles of the tongue.
Practically, all nerves, except for purely sensory nerves - 1 pair (olfactory) and 2 pairs (visual), receive innervation through that part of the pyramidal tract, which is called the corticonuclear, or corticonuclear. Then both already separated bundles pass past the inner capsule, where the conductors lie especially densely. This is the place of the highest con of the brain.
The internal capsule appears as a small band in the white matter that lies between the basal ganglia. In it, on a horizontal section, two “hips” are visible, tilted in different directions, and a “knee” connecting them. The corticonuclear tract is located in the “knee” region, and the corticospinal, pyramidal fascicle, which splits off above, occupies the anterior 2/3 of the “posterior thigh”.
After switching to the nuclei of the cranial nerves, the impulse goes further and, along individual nerves, approaches the corresponding muscles . Some of the beams also intersect and carry out movements on the opposite side, but some do not. In other words, part goes contralaterally, and part goes ipsilaterally.
The pyramid path itself
What about the main bundle, which should carry out movements to the arms and legs? It is still traveling in the depths of the brain, and as it moves towards the exit through the foramen magnum, it becomes denser and thicker.
After the axons leave the internal capsule, on the right and left these bundles pass through the middle of the cerebral peduncles and descend into the pons.
There, pyramidal tracts form each of the halves of the bridge, and go down, surrounded by a “retinue” of masses of bridge nuclei, fibers of the reticular formation and other formations.
Finally, leaving the pons and entering the medulla oblongata, the pyramidal tracts begin to become visible to the eye. Elongated and seemingly inverted pyramids appear, which are located symmetrically from the center. That is why the corresponding paths conducting movements are named this way.
Transition to the spinal cord
Having reached the bottom of the medulla oblongata, some of the axons cross over to the opposite side, as discussed above.
This crossed part forms the so-called lateral fasciculus, and the remaining uncrossed part is called the anterior corticospinal tract.
Surprisingly, the axons of the neurons of this bundle still move to the mirror side, but in the segment of the spinal cord that they should innervate. The transition occurs in the area of the white commissure anteriorly, which connects the right and left halves of the spinal cord.
The crossed, massive parts descend down, of course, not on their own, but as part of the same-named (tractus corticospinalis lateralis) path in the spinal cord.
As fibers are given off at the level of each segment, this bundle becomes thinner, like icicles “frozen” into the spinal cord on both sides.
Finally, in the region of the sacral region this bundle becomes very thin and ends.
Almost 90% of all fibers switch not directly to motor neurons in the greater horn of the spinal cord, but to interneurons . These neurons directly form synapses with large motor neurons, and differ from them in function.
We can say that the mass of interneurons, which are closed within one horizontal (segmental) level, are in contact with sensory and motor nerve cells, and have some autonomy. As a result, at the level of each segment there are polysynaptic “relay substations”.
This is what distinguishes the pyramidal and extrapyramidal pathways for regulating movements.
The extrapyramidal system, operating in a completely autonomous mode, does not require such a large number of two-way connections, since it is not accessible to voluntary control.
Instead of a conclusion
There are a few very important words left to say.
What happens if there is an obstacle in the way of the pyramidal beam? If axonal interruption occurs due to injury, will it cause their death or dysfunction (tumor, hemorrhage)? The result is paralysis of the muscle, which is left without a command to move.
Incomplete paralysis, in which some of the axons still “get” to the muscle, is called paresis, and is manifested by weakness and muscle wasting.
The most interesting thing is that when the central neuron dies or the path is interrupted, the second neuron remains unharmed - which lies in the anterior horns of the spinal cord and directly approaches the muscle. He just loses his “boss from above.” This type of paralysis is called central. And what happens as a result of central paralysis, why it occurs and how it manifests itself will definitely be discussed in the following articles
Pogrebnoy Stanislav Leonidovich, neurologist
Rate this article:
Total: 160
4.36 160
Source: https://mozgius.ru/stroenie/piramidnaya-sistema.html
Diagnosis of disorders
The descending pyramidal tract is a projection one, while the ascending tract is considered to be the one that transmits body signals through the spinal cord to the central nervous system. Descending, on the contrary, transmits brain signals to neurons.
To determine which system has been damaged and to what extent, during the examination, the neurologist examines many parameters relating to muscles, joints, and nerve reflexes.
A neurologist performs the following diagnostic procedures:
- examines the range of motion of all joints;
- checks deep reflexes, looks for pathological reflexes;
- checks the functioning of all facial nerves;
- measures electrical conductivity of muscles, their biopotentials;
- examines muscle strength;
- and is also required to check whether pathological clonic contractions are present.
When a neurologist checks range of motion, he begins by examining the larger joints first, and then examines the smaller ones. That is, first examines the shoulder joint, then the elbow and wrist.
Motor pyramidal tract. Symptoms of damage to the pyramidal tract
Our brain is a unique multi-complex system that simultaneously controls the sensory and vestibular apparatus, movement, thinking, speech, vision and much more.
In this article we will talk about how the brain controls voluntary and involuntary movement. And about what neurological abnormalities are associated with damage to the pyramidal system of the brain.
Pyramidal insufficiency in newborns. Causes
Symptoms of motor impairment in a child include strange jerking movements, or he may walk differently than other children - on tiptoe; or the placement of the feet is incorrect. The reasons for this condition in a child may be:
- underdevelopment of the brain (spinal or brain);
- birth trauma, if the parietal lobe of the brain or the brain stem itself is damaged, there will definitely be disturbances in the pyramidal tract;
- hereditary diseases of the nervous system.
- hypoxia;
- cerebral hemorrhage after childbirth;
- infection such as meningitis or arachnoiditis.
Treatment for adults is often medicinal. But for children it is much better to use methods such as exercise therapy, massage and taking vitamins. If there are no brain abscesses or other serious injuries, the condition improves by the first year of life.
Disturbance in the cervical spine leads to paresthesia. This is a neuropathy that is characterized by impaired sensitivity. A person may either lose touch sensation in the skin altogether or experience tingling sensations throughout the body. Paresthesia is treated with reflexology, manual therapy or physiotherapy. And, of course, you need to remove the main cause of neuropathy.
Another lesion of the pyramidal tracts and, consequently, motor activity is myoclonus - involuntary twitching.
There are several types of myoclonus:
- rhythmic myoclonic contractions of a separate muscle group;
- velopalatine contractions - sudden non-rhythmic contractions of the tongue or pharynx;
- postural myoclonus;
- cortical;
- myoclonus in response to physical activity (in athletes).
Myoclonus or cortical myoclonus is a disease of the nerve pathway caused by a disorder in the motor centers of the brain. That is, at the very beginning of the pyramid path. If there is a “failure” in the cortex, the signals reach the muscles already distorted.
However, the causes of disturbances in the motor pyramidal pathway can be a lack of magnesium, psycho-emotional or physical fatigue, and many other reasons. Therefore, the diagnosis must be made by a doctor after checking with an MRI.
Damage to the corticonuclear tract
The pyramidal path is the basis of all movements not only of the muscles of the body, but also of the face. The axons of various facial motor neurons transmit signals to the muscles. Let's take a closer look. The motor neurons of the nucleus ambiguus innervate the muscles of the pharynx, larynx, soft palate, and even the muscles of the upper esophagus.
Motor neurons of the trigeminal nerve are responsible for the work of some muscles of mastication and those that give the signal to the eardrum to contract. Individual motor neurons contract the facial muscles when we smile or frown. These are facial neurons.
Another group of muscles is responsible for eye and eyelid movements.
The defeat of the leading neuron affects the work of the “subordinate” muscles. The entire pyramidal path is based on this principle. Neurology of the facial nerve leads to very unpleasant consequences. However, eye movements and swallowing are usually preserved.
It is worth noting that complete disconnection of the facial muscles from the controlling segment of the brain occurs only if both the right and left hemispheres are affected. Most facial neurons are controlled bilaterally, as are the muscles of the trunk. One-way crossed fibers go only to the lower part of the face, namely to the muscles of the tongue and lower jaw.
Symptoms of damage to the pyramidal tract at the level of the brain stem
Since fiber crossover occurs at the level of the brain stem (the medulla oblongata and the pons), when these structures are damaged, gamiplasia occurs on the other half of the body. This symptom is called alternating paralysis.
The pyramidal tract is the basis of fine motor skills. If the brain stem is even slightly damaged, fine movements of the fingers are greatly affected.
There are many different syndromes that clearly and in detail characterize disorders that affect the work performed by the pyramidal tract: Avellis, Schmidt, Wallenberg-Zakharchenko syndromes and others. Based on the symptoms of these syndromes, the doctor can often determine the exact location of the pathway disorder before testing.
Source: https://FB.ru/article/324153/dvigatelnyiy-piramidnyiy-put-simptomyi-porajeniya-piramidnogo-puti
Neuropathology. Peripheral and central paralysis
Nerve fibers look like cords under a microscope. Their work is extremely important for the body. If conduction in some part of the nerve chain is disrupted, muscles in some parts of the body will not be able to receive signals. This will cause paralysis. Paralysis is divided into 2 types: central and peripheral.
If one of the central motor nerves in the “network” is disrupted, central paralysis occurs. And if there is a problem with the peripheral motor nerve, the paralysis will be peripheral.
With peripheral paralysis, the doctor observes a decrease in muscle tone and a severe decrease in muscle mass. Tendon reflexes will also be reduced or disappear completely.
The situation is different with central paralysis. Then hyperreflexia is observed, muscle tone is increased, and contractures are sometimes present.
Pyramidal neurons: functions and location in the brain
Neurons are the main type of cells that make up every element of the nervous system. These structures are well known to most people today.
But although in the collective imagination we have a typical idea or idea of what a neuron is, and many people imagine that all or almost all have the same structure and shape, the truth is that not all neurons are the same: there are very different types in depending on their shape, where they send information from, or even their relationship with other neurons. In this article we will focus on pyramidal neurons and their functions .
- Article on the topic: “Types of neurons: characteristics and functions
Pyramidal neurons
Pyramidal neurons are one of the different types of neurons present in our nervous system . They are one of the most common types of multipolar neurons, accounting for about 80% of the neurons in the cortex (not for nothing, the two layers of the cortex are called the inner and outer pyramids) and are found between some of the the most relevant from the body. They are generally considered to be projection neurons. That is, they operate by sending messages to cells that are far away and separated from the place where they were born.
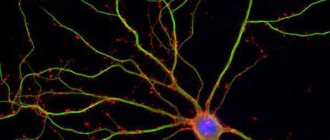
Discovered by Santiago Ramon y Cajal The name of this type of neuron refers to the shape of its soma, with a triangular or pyramidal appearance.
These are mainly glutamatergic neurons, with glutamate being the neurotransmitter that activates them, and they typically act as excitatory type neurons.
They can have different sizes, the largest of which are giant pyramidal cells or Betz cells.
Like other neurons, the structure of this type of neuron consists of a soma, which, as we have already said, has a pyramidal shape, an axon and dendrites. However, they have their own peculiarity: as for the dendrites, they are quite long compared to the rest, called the apical dendrite and numerous basal and shorter dendrites that branch.
- You may be interested in: “Parts of the Human Brain (and Functions)”
The location of these nerve cells
Pyramidal neurons can be found at various points in the nervous system, but they are much more common in some specific areas. Among them the following stand out.
Cortex
Pyramidal neurons are found primarily in the cerebral cortex, forming part of most of it, and are found in five of the six layers that make up this area of the brain. In particular, they can be observed in the granular and pyramidal layers, both external and internal.
They are especially prominent in the third and fifth layers (which are actually called the outer pyramidal and inner pyramidal), and they are larger the deeper into the cortex. There are also areas within the cortex where its existence has been discovered more frequently.
Motor cortex
In the motor cortex we can find a large number of pyramidal neurons, especially those associated with motor control. In this area of the cortex there are many giant pyramidal neurons known as Betz cells that transmit motor information from the brain to areas of the spinal cord, where they synapse with motor neurons that activate movement.
Prefrontal cortex
Pyramidal neurons can also be found in the prefrontal cortex, influencing higher mental processes. It is believed that these cells are the main primary excitations of prefrontal neurons, participating in numerous functions and considering themselves primordial for the existence of behavioral control.
Corticospinal tract
Pyramidal neurons are especially visible along the corticospinal tract, which sends motor information from different brain nuclei responsible for motor control to motor neurons that will cause muscle contraction as they pass through the spinal cord.
4. Hippocampus
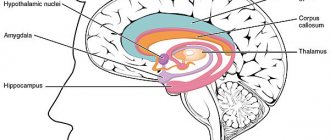
Not only in the cortex we can find pyramidal neurons, but we can also find in subcortical structures . One of them is the hippocampus, associated with aspects such as memory and orientation.
- Article on the topic: “Hippocampus: functions and structure of the memory organ”
5. Amygdala
Another structure in which these neurons are found is in the amygdala, an area of the limbic system associated with emotional memory.
Functions of pyramidal neurons
Like other neurons, pyramidal neurons are structures that transmit information in the form of electrochemical impulses that will be captured by other neurons until they reach their final destination. Being a type of neuron widely distributed in the cerebral cortex, pyramidal neurons are activated and connected to a large part functions and processes performed by humans. Examples of such functions are as follows.
1. Movement
Motor control is one of the functions that is traditionally associated with pyramidal neurons. In particular, these neurons are closely associated with voluntary motor control of muscles.
Cognition and executive functions
The excitatory role of pyramidal neurons in the prefrontal cortex means that their activation may be associated with cognitive processes of high importance, such as executive functions or cognition .
3. Emotions
The activity of pyramidal neurons in the prefrontal cortex is associated with the connection of these areas with various subcortical areas, among them the limbic . In this sense, the amygdala and hippocampus play a fundamental role.
Memory and orientation
Memory and specific orientation are other functions in which there is greater activation in pyramidal neurons, in this case in the hippocampus.
Bibliographical references
- Kandel E.R.; Schwartz, JH & Jessell, T.M. (2001). Principles of neurobiology. Fourth edition. McGraw-Hill Interamericana. Madrid.
- McDonald, A.J. (1992). Cell types and internal connections of the amygdala. Prog. Neurobiol. 55: 257-332.
Projection zones of the cerebral cortex
Projection (motor) zones of the cerebral cortex.
Direct irritation of certain areas of the cerebral cortex leads to muscle spasms corresponding to the area of the cortex - the projection motor zone. When the upper third of the anterior central gyrus is irritated, a muscle spasm occurs in the leg, middle arm, lower face, and on the side opposite to the source of irritation in the hemisphere. These seizures are called partial (Jacksonian). They were discovered by the English neurologist D.H. Jackson (1835-1911). In the projection motor zone of each cerebral hemisphere, all the muscles of the opposite half of the body are represented [2].
How to clean the inside of a stainless steel kettle from scale
To clean a regular or electric kettle, use Antiscale or Salit. But it is better to use food acids.
How to clean a metal kettle with lemon:
- Add a 25 gram packet of citric acid to 3 liters of water;
- Boil the solution for 15 minutes;
- After this, fill the container with plain water and boil again.
We invite you to familiarize yourself with Small white insects in the apartment and bathroom - photos, descriptions, how to get rid
Add a 25 gram packet of citric acid to 3 liters of water.
Potato or fruit peels containing organic acids are boiled inside a regular kettle. Brine or marinade from homemade or ready-made preserves works effectively. It contains vinegar, which destroys limescale.
Brine or marinade from homemade or ready-made preserves works effectively.
Scale is actively formed from tap water. If you fill it with filtered water, you will have to clean the dishes less often. You can use bottled water.
If you use filtered water, you will have to clean the dishes less often.