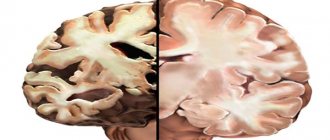
Puncture of the ventricles of the brain (ventricular puncture) is a surgical intervention that is carried out for diagnostic purposes (collecting cerebrospinal fluid for research) or for introducing medicinal or contrast agents into the ventricles of the brain. This surgical procedure allows you to diagnose various brain pathologies (abscesses, neoplasms, increased intracranial pressure, etc.) and prescribe the correct treatment.
Ventricular puncture is performed in an operating room using infiltration anesthesia or general anesthesia. There are no age restrictions for this surgical procedure. In most cases, the site of insertion of the puncture needle is the anterior or posterior horn of the lateral ventricle. The ventricles of the brain produce cerebrospinal fluid; their puncture makes it possible to identify the presence of many pathological processes in the brain. This surgical intervention is performed by a neurologist or neurosurgeon.
Areas of application, indications, contraindications
Such a study is carried out in areas where there is suspicion of pus formation, most often these are:
- lower part of the frontal lobe;
- inferior part of the temporal lobe;
- tympanic space;
- near the mastoid process.
A puncture is taken to diagnose brain pathologies, such as:
- infectious lesion of the central nervous system;
- inflammatory process in the central nervous system;
- bacterial, viral, fungal diseases;
- infection of brain tissue with tuberculosis or syphilis;
- bleeding;
- multiple sclerosis;
- neoplasms of any type;
- neuralgic pathologies;
- swelling of brain tissue;
- problems with the vascular system.
Important! Before the procedure, the patient must indicate in a special questionnaire a list of medications that he is currently taking, whether he is allergic to anesthetics or medications, and whether he has problems with blood clotting.
The procedure is prohibited if:
- the patient is at any stage of pregnancy;
- he is in a state of traumatic shock;
- lost a lot of blood;
- there are intracranial hematomas;
- brain abscess diagnosed;
- abundant;
- diagnosed with hypertension;
- there are abundant infectious and purulent lesions on the back;
- there are lumbar bedsores;
- the brain is injured.
Puncture of the posterior horn of the lateral ventricle
Position the patient on his stomach face down. The head should be positioned in such a way that the line of the zygomatic process of the temporal bone is strictly vertical, and the line of the sagittal suture is strictly in the median plane. The entire shaved scalp, forehead, ears, and back of the neck are treated twice with a solution of iodonate or iodopirone. A line of incision of the scalp is outlined with a 1% solution of brilliant green, which runs parallel to the sagittal suture through the Dandy point, dividing the incision line in half. Projection of the Dandy point on the scalp: 4 cm anteriorly and 3 cm outward from the external occipital tubercle of the skull, palpated through the soft integument of the head. The surgical field is limited to sterile linen. The incision of the soft covers of the head, the application of a burr hole, and the dissection of the dura mater are performed in exactly the same way as when accessing the anterior horn of the lateral ventricle. Needle 18, which punctures the ventricle, is inserted into the brain to a depth of 5-6 cm in the direction of the outer-superior corner of the orbit of the same side.
How to carry out the procedure
Why the procedure is being done has been determined, now you need to understand the methods for carrying it out. They are different and directly depend on the area where the liquid is taken.
Anterior horn of the lateral ventricle
The ventricular procedure for this area is performed as follows:
- The patient lies on his back when a tumor in the brain is to be identified. Usually the patient lies down on the healthy side to make it more convenient for the doctor to perform a puncture on the injured side.
- The head is slightly tilted towards the chest.
- The puncture site is thoroughly disinfected and coated with iodine twice.
- Draw a puncture line, which should be guided by the arrow-shaped seam, passing the Kocher point. It is covered with a layer of brilliant green solution.
- The head is covered with a sterile sheet.
- Any local anesthetic to which the patient is not allergic is used to numb the puncture area, most often it is Novocain.
- Using a scalpel, an incision is made along the intended line.
- A cut is made on the trepanation window on the exposed skull.
- The neurosurgeon makes a cross-shaped incision on the dura mater. Wax is rubbed in or electrocoagulation is performed. For what? To stop bleeding, the latter method being the most effective.
- The cannula is inserted into the brain tissue to a depth of no more than 5-6 cm so that it runs parallel to the incision line. When puncturing the wall of the lateral ventricle, the doctor will feel a slight dip.
- Yellowish cerebrospinal fluid will begin to flow through the submerged cannula. Having penetrated the cavity of the ventricle, the doctor fixes the needle and, using a mandrel, regulates the volume and speed of the withdrawn fluid.
Often there is high pressure in the ventricular cavity, and if it is not controlled, the fluid will flow out in a stream. This will lead to the patient developing neuralgic problems.
The permissible volume of fluid intake is in the range of 3-5 ml. It is important to note that in parallel with the preparation of the room for the puncture, the operating room is also prepared, since there is a high risk that air may enter the area being examined, or the depth of the puncture will be excessive, which may cause injury to the blood vessel. In these cases, the patient will be urgently operated on.
In cases of puncture, children use the methods of collecting cerebrospinal fluid according to Dogliotti and Geimanovich:
- In the first case, the puncture is carried out through the orbit.
- In the second - through the lower part of the temporal bone.
Both of these options have a significant difference from the traditional procedure - they can be repeated as often as necessary. For infants, this procedure is carried out through an open fontanel, simply by cutting the skin above it. In this case, there is a serious danger that the baby will develop a fistula.
Posterior horn of the brain
The technology for collecting cerebrospinal fluid from the area is carried out in the following order:
- The patient lies on his stomach. His head is tightly fixed so that the sagittal suture is strictly in the middle cavity.
- The preparatory process is identical to the above procedure.
- The incision of the skull tissue is carried out parallel to the sagittal suture, but so that it passes through the Dandy point, which should be strictly in its middle.
- Take a needle number 18, which is used strictly for this type of puncture.
- It is inserted at an angle, directing the needle tip into the outer upper edge of the orbit to a depth of no more than 7 cm. If the procedure is performed on a child, the puncture depth should not exceed 3 cm.
inferior horn of the brain
The principle of the procedure is similar to the previous two:
- the patient should lie on his side, since the surgical field will be the side of the head and the auricle;
- the incision line will go 3.5 cm from the external auditory canal and 3 cm above it;
- part of the bone in this area will be removed;
- an incision will be made in the dura mater of the brain;
- insert a puncture needle 4 cm, directing it to the top of the auricle;
- cerebrospinal fluid will be collected.
How to take a puncture
To avoid damaging the spinal cord, the puncture is taken between the second and third lumbar vertebrae in adults, and between the third and fourth in children. This is explained by the fact that the spinal cord in adults usually extends to the level of the second vertebra, and in children it may extend lower - to the third.
For this reason, spinal cord puncture is also called lumbar puncture.
To carry out the puncture, special long Beer needles of reinforced design (thick-walled) with a mandrin (stiletto) are used.
Preparation for puncture
Before collecting cerebrospinal fluid for analysis, it is necessary to conduct an examination:
- pass general and biochemical blood and urine tests;
- do a blood coagulogram;
- change fundus pressure and intracranial pressure;
- for neurological disorders, cerebral signs indicating dislocations - CT or MRI of the brain;
- other tests prescribed by your doctor.
How is a spinal cord puncture performed?
- The patient lies on his side on a hard couch, bending his knees to his stomach and bending his back as much as possible. A sitting position is also allowed.
- The surface of the lower back is treated with iodine solution.
- The needle is inserted into the intervertebral space between the second and third (third and fourth in children) vertebrae, at the level of the spinous processes, slightly at an upward angle.
- At the beginning of the needle's advancement, an obstacle is soon felt (these are the vertebral ligaments), but when 4 to 7 cm have been passed (about 2 cm in children), the needle falls under the arachnoid membrane and then moves freely.
- At this level, the progress stops, the mandrin is removed, and by the flow of drops of colorless liquid from it, it is confirmed that the goal has been achieved.
- If the liquid does not drip, and the needle rests on something hard, it is carefully returned back without completely removing it from the subcutaneous layer, and the injection is repeated, slightly changing the angle.
- Cerebrospinal fluid is collected in a test tube; the volume of the sample is 120 g.
- If you need to examine the epidural space to see adhesions and tumors, or the condition of the spinal ligaments, a three-channel test is performed (saline is supplied through one channel, a needle with a catheter is supplied through the second, and a micro-camera for viewing is supplied through the third).
- Anesthesia or therapy is administered by administering an anesthetic or medicinal drug through a catheter.
After the puncture, the patient turns over on his stomach and remains in this position for at least three hours. You absolutely cannot get up right away! This is necessary to prevent the development of complications.
Does it hurt when taking a puncture?
Many patients are afraid that it will hurt. You can calm them down: before the analysis itself, local anesthesia is usually performed: layer-by-layer injection of novocaine (1 - 2%) into the area of the future puncture. And even if the doctor decides that local anesthesia is not needed, in general the puncture is no more painful than a regular injection.
Complications and consequences of spinal cord puncture
After the puncture, the following complications are possible:
- On the membranes of the spinal cord, when subcutaneous epithelial cells are introduced with a needle, the development of an epithelial tumor - cholesteatoma - is possible.
- Due to a decrease in the volume of cerebrospinal fluid (daily circulation volume - 0.5 l), intracranial pressure decreases, and a headache may occur for a week.
- If nerves or blood vessels are damaged during a puncture, the consequences can be very unpleasant: pain, loss of sensitivity; formation of hematoma, epidural abscess.
However, such phenomena are extremely rare, since spinal puncture is usually performed by experienced neurosurgeons with experience in numerous operations.
Shoshina Vera Nikolaevna
Therapist, education: Northern Medical University. Work experience 10 years.
Articles written
For many, brain puncture is subconsciously considered dangerous, but in fact it is not. If performed by an experienced doctor, it is absolutely safe. It is thanks to it that it is possible to detect ulcers in brain tissue, determine the contents of neoplasms and the state of other pathologies.
But there are also a number of dangers that can be encountered with this procedure. Let's figure it out.
The puncture is performed with a special needle, which, penetrating the brain tissue, can draw fluid from it. To make a puncture safe, you need to follow a number of rules:
- The area of the head where the puncture will be made must be thoroughly disinfected. First, it is treated with hydrogen peroxide, and then generously lubricated with iodine.
- For the procedure, you cannot use a regular needle, only a special puncture needle with a blunt end. It is produced quite wide and equipped with a mandrel.
- There should be 2 needles, one of which will be a spare if the first one is blocked by brain tissue.
- The puncture should be made to a depth of no more than 4 cm. This is the only way to ensure the safety of the fence and prevent the penetration of purulent secretions into.
- Before the procedure, the patient must have a bowel movement.
- The patient must be completely immobile, so he can be fixed with special devices.
Clinical picture after the procedure
Of course, the symptoms after puncture sampling are different for everyone, but they can be combined into a general clinical picture:
- Pain in the head area of varying intensity and duration.
- Prolonged nausea and vomiting.
- Convulsions and fainting.
- Malfunction of the cardiovascular system.
- Impaired respiratory function; in rare cases, the patient may need artificial ventilation.
- Neuralgic problems.
Whether the patient will have the above symptoms directly depends on the experience of the neurosurgeon and his skills. The procedure must be performed strictly according to medical instructions, which can guarantee the absence of complications after the puncture.
It is important not only to correctly fix the patient, but also to accurately determine the puncture area. Treatment of the affected area is important both at the stage of preparation for the procedure and after it. Upon completion of the collection, be sure to apply a sterile bandage.
It is important that the patient does not feel any discomfort, much less pain, at the time of the puncture.
Due to the fact that the procedure is most often prescribed for diagnosing pathologies, it, like any other diagnostic measure, should be painless. The patient will be conscious at all times, so he should immediately inform the doctor about any discomfort that has arisen. This will help avoid a number of complications. The doctor will change the technology or completely interrupt the procedure.
Puncture is an important procedure in medicine, and taking cerebrospinal fluid from the brain is even more important. Before undergoing it, the patient will undergo a series of studies that will help identify possible contraindications. There is no need to worry; brain puncture is performed only by experienced specialists who know their job.
(ventricular puncture) is a diagnostic operation that is performed to obtain intraventricular cerebrospinal fluid, examine the ventricles of the brain using a ventriculoscope or contrast. Ventricular puncture makes it possible to diagnose tumor and purulent processes, increased intracranial pressure, and intraventricular bleeding. It can be performed for both diagnostic and therapeutic purposes (to stop bleeding, provide artificial drainage). Puncture of the ventricles of the brain is carried out through a small burr hole in the bones of the skull.
Links
Wikimedia Foundation. 2010.
- Ventry
- Vyanta eldership
See what “Ventricular puncture” is in other dictionaries:
- PUNCTURE
- (punctio), puncture of the cavity with a syringe containing diagnostic or therapeutic. purpose. P. is used for emptying various kinds of liquids and gases from tissues and cavities (emptying P.), determining their presence (test P.), for bacterial, chemical. And… …
ventricular puncture
- (p. ventricularis) P. ventricles of the brain ... Big Medical Dictionary
Hydrocephalus
— Skull of a patient with hydrocephalus... Wikipedia
Intracranial hematoma
— Intracranial hematoma is a pathological formation that is a hematoma widespread within the cranial cavity. The incidence of intracranial hematomas is 12–13% of neurosurgical patients. Contents 1 Etiology 2 ... ... Wikipedia
HEART
- HEART. Contents: I. Comparative anatomy……….. 162 II. Anatomy and histology……….. 167 III. Comparative physiology………. 183 IV. Physiology………………. 188 V. Pathophysiology……………. 207 VI. Physiology, pat.... ...Big Medical Encyclopedia
Cerebrospinal fluid
— Pulsation of the cerebrospinal fluid during heartbeat Cerebrospinal fluid, cerebrospinal fluid (lat. liquor cerebrospinalis), cerebrospinal fluid is a fluid constantly circulating in the ventricles of the brain, cerebrospinal fluid... Wikipedia
HEART
- Rice. 1. The heart of various animals. Rice. 1. Heart of various animals: 1 - cattle (front view); 2 — horses (rear view); 3 — pigs (front view); 4 — sheep (rear view); 5 — dogs (left view); 6 —… … Veterinary encyclopedic dictionary
Shoshina Vera Nikolaevna
Therapist, education: Northern Medical University. Work experience 10 years.
Articles written
For many, brain puncture is subconsciously considered dangerous, but in fact it is not. If performed by an experienced doctor, it is absolutely safe. It is thanks to it that it is possible to detect ulcers in brain tissue, determine the contents of neoplasms and the state of other pathologies.
But there are also a number of dangers that can be encountered with this procedure. Let's figure it out.
The puncture is performed with a special needle, which, penetrating the brain tissue, can draw fluid from it. To make a puncture safe, you need to follow a number of rules:
- The area of the head where the puncture will be made must be thoroughly disinfected. First, it is treated with hydrogen peroxide, and then generously lubricated with iodine.
- For the procedure, you cannot use a regular needle, only a special puncture needle with a blunt end. It is produced quite wide and equipped with a mandrel.
- There should be 2 needles, one of which will be a spare if the first one is blocked by brain tissue.
- The puncture should be made to a depth of no more than 4 cm. This is the only way to ensure the safety of the fence and prevent the penetration of purulent secretions into.
- Before the procedure, the patient must have a bowel movement.
- The patient must be completely immobile, so he can be fixed with special devices.
Indications
Most often, ventricular puncture in neurology is prescribed when a tumor process is suspected, which cannot be accurately diagnosed using CT or MRI of the brain. Studying the fluid obtained during puncture and tomography of the ventricles after the administration of contrast make it possible to clarify the diagnosis, determine the type of neoplasm and prescribe adequate treatment. For patients with suspected intraventricular hemorrhage, ventricular puncture is performed not only for diagnostic purposes, but also for therapeutic purposes (intraventricular administration of drugs to stop bleeding). The technique is also used to insert a ventriculoscope to examine the ventricle or perform surgery. During the manipulation, if necessary, an emergency reduction of intracranial pressure and installation of a ventricular drainage system is carried out.
Types of diagnostics
Before performing a biopsy of a tumor located in the brain, diagnostic studies are performed, including neuroimaging (CT, MRI), electroencephalography, if necessary, angiography (a study of the circulatory system of the brain) and ventriculography (a study of the ventricular system of the brain). There are different types of biopsy:
- Open. It is performed during a neurosurgical operation through a craniotomy to remove the tumor.
- Stereotactic. Minimally invasive intervention is performed using a stereotactic frame or navigation system.
- Puncture. A needle is inserted through a hole in the skull bone into the brain tissue, and a small piece of brain matter is removed.
Among all types, open biopsy in the brain area is performed more often than others and is associated with the greatest risk of injury and complications. The high frequency of use is associated with the mandatory removal of a fragment of material during surgery to remove an intracranial tumor. An open diagnostic procedure is performed under general anesthesia in parallel with the main operation.
Stereotactic biopsy is the second most frequently performed biopsy if there is a suspicion of the development of a tumor in the brain. This method is chosen when, due to the inaccessible location of the lesion or the serious condition of the patient, it is impossible to perform a full-fledged operation to remove the tumor. It is considered an informative and safest research method.
Methodology
Most often, the lateral ventricle is punctured for diagnostic purposes. In children with an open large fontanel, a puncture is performed through the skin with a regular surgical needle in the outer corner of the fontanel. When the fontanelle is closed, a loose coronal suture can be used to insert the needle. In adults, puncture of the lateral ventricle is performed through its anterior or posterior horn. When puncturing the anterior horn, the puncture site is determined by focusing on the midline of the skull, connecting the bridge of the nose and the back of the head. A 4 cm incision is made 8-9 cm above the brow ridge and 2 cm outwards from this line. When puncturing the posterior horn, the incision passes 3 cm above and outward from the occipital protuberance. Next, a special cutter is used to make a hole in the skull, dissect the dura mater and insert a cannula - a hollow metal tube with a curved end to remove fluid located in the ventricular cavity.
The cannula is advanced to a depth of 5-6 cm. When it reaches the ventricle, the doctor removes the mandrel, and intraventricular cerebrospinal fluid (CSF) begins to drip from the outer end of the cannula. The rate of fluid flow can be used to judge the magnitude of the liquor pressure. To accurately determine it, the cannula is connected to a pressure gauge. Normally, the pressure in the patient's lying position is 110-160 mmH2O. Art., in a sitting position - 240-280 mm of water. Art. If necessary, the required amount of cerebrospinal fluid is removed or a contrast agent is injected and a series of tomograms are made. Then the cannula is removed and the wound is sutured.
Already in the process of collecting cerebrospinal fluid, the doctor can assess its color (normally transparent). When hemorrhaging into the ventricles, the fluid contains an admixture of blood; its color can be used to judge the time that has passed since the bleeding. During purulent processes or breakthrough of pus from an abscess into the ventricular system, the liquid has a greenish tint and an unpleasant odor. The cerebrospinal fluid taken as a sample is sent to the laboratory for detailed study. There they determine its density, pH, composition, and conduct a study for the presence of viruses and bacteria. A detailed description of the study of cerebrospinal fluid is presented here.
Brain puncture
is not a dangerous procedure.
It is carried out to detect abscesses in the brain.
complications are possible during a brain puncture This is an infection in the brain; vascular damage; penetration of pus into the ventricles of the brain.
Technique
Most often, puncture of the anterior or posterior horn of the lateral ventricle is performed.
When puncturing the anterior horn of the lateral ventricle, a linear soft tissue incision about 4 cm long is made. The edges of the skin are separated using a Jansen retractor. A burr hole is placed at Kocher's point, which should be located 2 cm anterior to the coronal suture and 2 cm lateral to the midline of the sagittal suture. The dura mater is opened crosswise and a cannula is inserted into the brain for ventriculopuncture. The cannula is advanced parallel to the sagittal plane in the direction of the internal auditory canal. Normally, in adults, the anterior horn is located at a depth of 5-5.5 cm. With hydrocephalus, this distance can be significantly reduced. To puncture the posterior horn, a burr hole is placed at the Dandy point 3 cm lateral and 3 cm above the external occipital protuberance. The cannulas are immersed into the brain in the direction of the upper outer edge of the orbit. Normally, the posterior horn is located at a depth of 6-7 cm.
Purpose of a spinal tap
Spinal cord puncture is performed for:
Performing a spinal tap
- collecting a small amount of cerebrospinal fluid (CSF). Subsequently, their histology is carried out;
- measuring the pressure of cerebrospinal fluid in the spinal canal;
- removal of excess cerebrospinal fluid;
- administration of drugs into the spinal canal;
- relief of difficult labor in order to prevent painful shock, as well as as anesthesia before surgery;
- determining the nature of the stroke;
- isolation of tumor markers;
- performing cisternography and myelography.
Using a spinal tap, the following diseases are diagnosed:
- bacterial, fungal and viral infections (meningitis, encephalitis, syphilis, arachnoiditis);
- subarachnoid bleeding (bleeding in the brain);
- malignant tumors of the brain and spinal cord;
- inflammatory conditions of the nervous system (Guillain-Barré syndrome, multiple sclerosis);
- autoimmune and dystrophic processes.
Often a spinal tap is equated with a bone marrow biopsy, but this statement is not entirely correct. During a biopsy, a tissue sample is taken for further research. Access to the bone marrow is achieved through a puncture of the sternum. This method allows you to identify bone marrow pathologies, some blood diseases (anemia, leukocytosis and others), as well as metastases in the bone marrow. In some cases, a biopsy can be performed during the puncture process.
To prevent and treat JOINT DISEASES, our regular reader uses the increasingly popular NON-SURGERY treatment method recommended by leading German and Israeli orthopedists. After carefully reviewing it, we decided to offer it to your attention.
What are the consequences of puncture?
- One of the most common consequences resulting from this procedure is headache.
Begins in the period from twelve to 20 four hours from the moment of completion of the procedure.Its duration ranges from a couple of days to fourteen days. The pain tends to decrease in intensity in a horizontal position of the body and increase in a vertical position.
- Bleeding occurs especially often when taking anticoagulants.
- Various types of hematoma.
- Damage to the intervertebral disc or nerve roots by a needle.
- When skin particles enter the cerebrospinal fluid, tumors of the spinal canal are formed.
- The introduction of drugs, contrast, and antibacterial agents into the spinal space entails a change in the composition of the cerebrospinal fluid. Myelitis, arachnoiditis or radiculitis may develop.
- Miscarriages are common in the first trimester of pregnancy.
The risks and benefits of performing a lumbar puncture are carefully considered and decided after all possible studies have been performed.
Specifically taking into account the clinical manifestations of each patient. The final decision rests with the patient or his relatives. In the days of MRI and CT, this manipulation began to be used less frequently. But for some diseases it is indispensable.
Indications for spinal cord puncture
Spinal cord puncture is mandatory for infectious diseases, hemorrhages, and malignant neoplasms.
Inflammatory polyneuropathy
A puncture is taken in some cases for relative indications:
- inflammatory polyneuropathy;
- fever of unknown pathogenesis;
- demyelinating diseases (multiple sclerosis);
- systemic connective tissue diseases.
Preparatory stage
Before the procedure, medical workers explain to the patient why the puncture is being performed, how to behave during the procedure, how to prepare for it, as well as possible risks and complications.
Spinal cord puncture requires the following preparation:
- Registration of written consent for the manipulation.
- Taking blood tests to evaluate blood clotting, as well as the functioning of the kidneys and liver.
- Hydrocephalus and some other diseases require computed tomography and MRI of the brain.
- Collection of information on the medical history, recent and chronic pathological processes.
The specialist must be informed about the medications the patient is taking, especially those that thin the blood (Warfarin, Heparin), relieve pain, or have an anti-inflammatory effect (Aspirin, Ibuprofen). The doctor should be aware of existing allergic reactions caused by local anesthetics, anesthesia drugs, iodine-containing agents (Novocaine, Lidocaine, iodine, alcohol), as well as contrast agents.
It is necessary to stop taking blood thinning drugs, as well as analgesics and non-steroidal anti-inflammatory drugs in advance.
Before the procedure, water and food are not consumed for 12 hours.
Women must provide information about their suspected pregnancy. This information is necessary due to the expected x-ray examination during the procedure and the use of anesthetics, which may have an undesirable effect on the unborn child.
Your doctor may prescribe a medication to take before the procedure.
The presence of a person who will be next to the patient is mandatory. A child is allowed to undergo a spinal puncture in the presence of his mother or father.
Technique of the procedure
A spinal cord puncture is performed in a hospital ward or treatment room. Before the procedure, the patient empties his bladder and changes into hospital clothes.
Spinal cord puncture
The patient lies on his side, bends his legs and presses them to his stomach. The neck should also be in a bent position, with the chin pressed to the chest. In some cases, spinal puncture is performed with the patient sitting. The back should be as motionless as possible.
The skin in the puncture area is cleaned of hair, disinfected and covered with a sterile napkin.
The specialist may use general anesthesia or use a local anesthetic. In some cases, a drug with a sedative effect may be used. Also during the procedure, heartbeat, pulse and blood pressure are monitored.
The histological structure of the spinal cord provides for the safest needle insertion between the 3rd and 4th or 4th and 5th lumbar vertebrae. Fluoroscopy allows you to display a video image on a monitor and monitor the manipulation process.
Next, the specialist collects cerebrospinal fluid for further research, removes excess cerebrospinal fluid or injects the necessary drug. The liquid is released without outside help and fills the test tube drop by drop. Next, the needle is removed and the skin is covered with a bandage.
CSF samples are sent for laboratory testing, where histology occurs directly.
Spinal cord cerebrospinal fluid
The doctor begins to draw conclusions based on the nature of the fluid coming out and its appearance. In its normal state, the cerebrospinal fluid is transparent and flows out one drop per second.
At the end of the procedure you must:
- adherence to bed rest for 3 to 5 days as recommended by a doctor;
- keeping the body in a horizontal position for at least three hours;
- getting rid of physical activity.
When the puncture site is very painful, you can resort to painkillers.
Puncture of the anterior horn of the lateral ventricle
Position the patient on his back, face up. After treating the scalp twice with a solution of iodonate or iodopyrone, a 1% solution of brilliant green is used to mark a cut line for the soft tissues of the head, running parallel to the sagittal suture through the Kocher point, dividing the cut line in half. Projection of Kocher's point on the scalp: 2 cm anteriorly and 2 cm outward from the intersection of the sagittal and coronal sutures of the skull, which are determined by palpation through the scalp or restoration of a perpendicular line from the middle of the zygomatic arch to the intersection with the sagittal suture. The surgical field is then isolated with a sterile drape. The edges of the wound are moved apart with a Jansen retractor, a burr hole is made with a large cutter, and the remnants of the vitreous plate are removed with a Volkmann spoon. Bleeding from the bone is stopped by rubbing wax into the bone. Visible vessels of the dura mater are coagulated, and it is dissected crosswise. The vessels of the choroid of the brain are coagulated. A spinal puncture needle (or a special cerebral cannula) is inserted into the brain to a depth of 4.5-5.5 cm parallel to the median plane on a mentally drawn line connecting both auditory canals (biauricular line). When the needle enters the cavity of the lateral ventricle, ventricular fluid begins to flow from it. In this position, the needle is fixed with a rubber retainer, gauze balls and other methods so that it does not move. Fluid is removed from the ventricle slowly under the control of a removed mandrel.
Risks
Adverse consequences after spinal cord puncture occur in 1–5 cases out of 1000. There is a risk of:
Intervertebral hernia
- axial wedging;
- meningism (symptoms of meningitis occur in the absence of an inflammatory process);
- infectious diseases of the central nervous system;
- severe headache, nausea, vomiting, dizziness. Your head may hurt for several days;
- damage to the spinal cord roots;
- bleeding;
- intervertebral hernia;
- epidermoid cyst;
- meningeal reaction.
If the consequences of the puncture are expressed in chills, numbness, fever, a feeling of tightness in the neck, or discharge at the puncture site, you should immediately consult a doctor.
There is an opinion that during a spinal tap the spinal cord can be damaged. It is erroneous, since the spinal cord is located higher than the lumbar spine, where the puncture is directly made.
Puncture of the inferior horn of the lateral ventricle
Position the patient lying on his side. The scalp and auricle are treated twice with a solution of iodonate or iodopirone. A line of incision of the scalp is outlined with a 1% solution of brilliant green, passing in the vertical direction through the Keene point, dividing the incision line in half. Projection of the point on the scalp: 3 cm above and 3 cm posterior to the opening of the external auditory canal. The surgical field is limited to sterile linen. The incision of the soft covers of the head, the application of a burr hole, and the dissection of the dura mater are performed in the same way as when accessing the anterior horn of the lateral ventricle. The needle used to puncture the ventricle is inserted towards the upper edge of the opposite auricle to a depth of 4-4.5 cm.
Contraindications to spinal cord puncture
Spinal cord puncture, like many research methods, has contraindications. Puncture is prohibited in case of sharply increased intracranial pressure, dropsy or cerebral edema, or the presence of various formations in the brain.
It is not recommended to take a puncture if there are pustular rashes in the lumbar region, pregnancy, impaired blood clotting, taking blood thinning drugs, or ruptured aneurysms of the brain or spinal cord.
In each individual case, the doctor must analyze in detail the risk of the manipulation and its consequences for the life and health of the patient.
It is advisable to contact an experienced doctor who will not only explain in detail why it is necessary to perform a spinal cord puncture, but will also carry out the procedure with minimal risk to the patient’s health.
Preparation stage
https://www.youtube.com/watch?v=WuSIRjAsusc
The lumbar puncture procedure requires preliminary preparation. First of all, the patient is prescribed general clinical and biochemical blood and urine tests, and the state of the blood coagulation system is necessarily determined. The lumbar spine is examined and palpated. To identify possible deformations that may interfere with the puncture.
You need to tell your doctor about all the medications you are currently taking or have recently taken. Particular attention should be paid to drugs that affect blood clotting (aspirin, warfarin, clopidogrel, heparin and other antiplatelet agents and anticoagulants, non-steroidal anti-inflammatory drugs).
You also need to inform the doctor about possible allergies to medications, including anesthetics and contrast agents, recent acute illnesses, or the presence of chronic illnesses, as some of them may be a contraindication to the study. All women of childbearing age should tell their doctor if they may be pregnant.
Before performing a spinal cord puncture, the patient must consult a doctor.
It is forbidden to eat for 12 hours before the procedure and drink for 4 hours before the puncture.
To understand how a biopsy is done in the brain area, you need to get an idea of the procedure. The preparatory stage includes a comprehensive examination, including laboratory tests, consultations with a cardiologist, phlebologist, and anesthesiologist. Several hours before the intervention, the patient does not take food or water.
It is important to promptly inform your doctor about any allergies to medications and regular use of medications that prevent blood clots. If the patient is taking thrombolytics before an invasive diagnostic test, therapy is temporarily suspended. Stages of the open procedure:
- Making an incision on the scalp.
- Formation of a hole in the skull.
- Removal of a fragment of skull bone tissue to form a trepanation window.
- Peeling of the meninges.
- Resection (partial or complete removal) of the tumor.
- Closing the trepanation window with bone tissue or a special plate.
After completion of neurosurgical procedures, a sample of neoplasm tissue is sent to the laboratory to study the cellular structure. The stages of performing a stereotactic biopsy in the brain region depend on the type of equipment used. The sequence of manipulations when using a coordinating stereotactic frame:
- The exact localization of the pathological focus is determined using neuroimaging (mainly MRI).
- Local anesthetics or general anesthesia are used.
- A stereotaxic frame is installed in the head area.
- An MRI localizer with contrast marks is attached (a special device for limiting the area of intervention).
- A CT scan is performed.
- The results of MRI and CT studies are combined to achieve maximum accuracy when creating injection points.
- An incision is made into the skin of the head.
- A hole is drilled in the skull bone.
- A needle is inserted and moves under the control of an MRI or CT diagnostic complex.
- Material is being collected.
A study using a frame allows you to precisely approach the site of a tumor or other pathological process with an accuracy of 1 mm. The duration of the intervention is about 6 hours. One day after completion of the procedure, the patient is discharged from the hospital. Sequence of manipulations when using the navigation system:
- A study is carried out in MRI or CT format to obtain information such as the structural features of the patient’s brain, the location and size of the pathological focus.
- Neuroimaging results are transferred to the navigation system.
- A model of the brain is created in 3D projection.
- The image is studied to determine the optimal insertion point and needle trajectory.
- Anesthetics are administered to the patient.
- An incision is made on the skin of the head.
- A diagnostic hole is formed.
- Under the control of a navigation system, a puncture needle equipped with a camera and LED illumination is inserted into the cavity of the skull.
- Material is being collected.
A brain biopsy using a navigation system is carried out with minimal negative impact on healthy brain tissue, because calculations such as the shortest and safest path to the tumor site are previously performed. The doctor has the opportunity to choose a trajectory that goes around the areas responsible for vital functions, thereby significantly reducing the risk of complications.
The procedure time for a biopsy in the brain area using a navigation system is significantly reduced compared to intervention using a stereotactic frame. Reducing the duration of the procedure is associated with preliminary planning of actions.
During a puncture biopsy, an incision is made on the skin in the projection where the tumor is localized. Through a hole drilled in the skull bone, a puncture needle is inserted into the pathological focus to obtain a sample of the material. The stereotactic and puncture-type procedure is associated with minimal damage to the medulla, meninges, and bone tissue.
Hearing impairment
Although subclinical or even clinically detectable hearing loss after spinal anesthesia has long been known, few young anesthesiologists are aware of this possibility. Some authors believe that, for legal reasons, patients should be warned about this before spinal anesthesia, others believe that this will only lead to unnecessary fear.
Frequency . Clinically significant subjective hearing impairment: decreased hearing, ringing, buzzing or buzzing in the ears was detected (without audiometry) in 0.4% of patients after 9277 spinal anesthesias. Audiometrically, hearing loss in one or both ears is detected in 10-50% of patients, but a clinically noticeable decrease is detected in less than a quarter of these 10-50%.
Mechanism . The cause of hearing loss, as well as post-puncture headache, is liquor hypotension. The endolymph of the cochlea of the inner ear communicates with the subdural space of the brain, and the perilymph communicates with the subarachnoid space of the brain. Liqueur hypotension after spinal puncture disrupts the functioning of the organ of Corti.
Risk factors are the same as for post-puncture headache: patient age, needle gauge and model.
Why are hearing impairments less common than post-dural puncture headaches? Because, firstly, these disorders can be subclinical, and secondly, 7% of adults have anatomical obstruction of the cochlear aqueduct, and 30% have functional obstruction. In them, changes in liquor pressure are not transmitted to the perilymph. This also explains cases of unilateral hearing impairment.
Clinical manifestations : hearing loss, ringing, buzzing or buzzing in the ears are rare. With pure tone audiometry, hearing loss is detected much more often, and more so in the low frequency range, which is explained by the thinner thickness and greater compliance of the basement membrane closer to the apex of the cochlea, where transduction of low-frequency sounds occurs.
Differential diagnosis . Accidental puncture of the membranes of the spinal cord or brain as a cause of hearing impairment is possible with interscalene blockade of the brachial plexus, alveolar or infiltration blockade in dentistry.
Meniere's syndrome (endolymphatic hydrops) is also manifested by ringing or noise in the ears and hearing loss (the mechanism is similar, but the basement membrane of the cochlea is displaced not due to low perilymph pressure, but due to high endolymph pressure), but vestibular disorders appear earlier and are more pronounced .
Ear surgery and any surgery performed under general anesthesia, especially with cardiopulmonary bypass, can also cause hearing problems.
Ototoxicity is inherent in a number of medications: loop diuretics (furosemide, bumetanide, ethacrynic acid), antibiotics (aminoglycosides, erythromycin, vancomycin), aspirin, non-steroidal anti-inflammatory drugs (ketorolac, naproxen, piroxicam), antitumor drugs (cisplatin, vincristine, vinblastine).
Treatment : elimination of liquor hypotension (as with post-puncture headache). Epidural filling with autologous blood is usually effective.
Forecast . Hearing impairment after spinal puncture disappears without a trace in more than 95% of cases. Irreversible damage is very rare.