An aneurysm is a small, unnatural formation that is located on the wall of blood vessels in the brain. It tends to quickly increase in size and fill with blood. According to official statistics, this pathology is found in every 17th person in the world. Most often it is observed in people between 40 and 60 years old. More than 50% of patients die within 30-40 days after aneurysm rupture. In patients who survive after surgery for cerebral aneurysm, various neurological disorders are subsequently observed.
Causes
A combination of genetic and environmental factors leads to the development of a cerebral aneurysm.
For example, people with congenital polycystic kidney disease and arteriovenous malformations are more likely to develop the disease. Other reasons include:
- Smoking tobacco;
- Heredity;
- High blood pressure;
- Overweight;
- Poor diet (excessive salt intake, lack of fruits and vegetables);
- Lack of physical activity;
- High caffeine consumption;
- Excessive alcohol consumption;
- Age over 40 years;
- Gender – Women are more likely to develop a brain aneurysm than men. This may be due to decreased levels of the hormone estrogen after menopause. Estrogen helps maintain the elasticity of blood vessels;
- Pre-existing weakness of blood vessels;
- Severe traumatic brain injury;
- Cocaine abuse;
- Autosomal dominant polycystic kidney disease is a genetic disease that causes the development of multiple cysts on the kidneys;
- Connective tissue disorders – Ehlers-Danlos syndrome or Marfan syndrome;
- Coarctation of the aorta is a congenital heart defect.
Elena Malysheva about aneurysm rupture
Consequences and complications
Immediate complications:
- Leakage or rupture of anastomosis;
- Infection;
- Repeated bleeding;
- Stroke;
- Hydrocephalus.
Long-term consequences:
- Anastomotic thrombosis;
- Decreased vision, hearing;
- Neurological deficits (decrease in cognitive functions and socialization, personality changes);
- Recurrence of aneurysm.
Prevention methods:
- Bed rest until clinical improvement;
- Physical and emotional peace;
- Taking antihypertensive drugs, statins, antiplatelet agents and anticoagulants;
- If the condition worsens, contact your doctor.
How does a breakup happen?
An aneurysm is a bulge in the arterial wall. As the bulge grows, it becomes thinner and weaker, and the increased blood pressure inside it can cause it to rupture. Aneurysms usually develop on large blood vessels where they branch. Approximately 80% of aneurysms form in the front of the brain, and 20% in the back. Aneurysms are:
- Saccular (saccular) - the most common type, also called “berry”, such an aneurysm protrudes from one side of the artery and has a pronounced isthmus at the base, there are usually no symptoms of this form of aneurysm;
- Fusiform - the aneurysm protrudes in all directions and does not have a distinct isthmus;
- Giant - saccular or fusiform more than 2.5 cm in diameter, have a wide isthmus and can affect more than one artery, symptoms are pronounced;
- Traumatic – caused by a closed head injury, causing severe symptoms, including headache and general malaise.
fatal in 50% of cases .
Excess blood in the subarachnoid space increases pressure on the brain. And the area of the brain that previously received oxygenated blood from the affected artery is now deprived of it, which leads to a stroke or causes symptoms of tachycardia.
Complications
- Vasospasm is a complication that manifests itself 5-10 days after the rupture. The condition causes symptoms such as spasm and narrowing of the walls of blood vessels, blood flow to the brain area decreases, which causes a secondary stroke;
- Further, interrupted blood flow can cause further brain damage and cause ischemic stroke ;
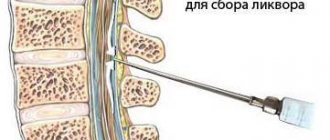
- Another serious complication of subarachnoid hemorrhage is hydrocephalus - excessive accumulation of cerebrospinal fluid in the skull dilates the ventricles, which begin to put pressure on the brain tissue;
- Bleeding in the brain can cause the formation of a hematoma , which can only be removed surgically.
Other complications include:
- Thromboembolism – acute blockage of blood vessels;
- Angina;
- Strong headache;
- Aortic dissection (occurs in a bulging part of the artery as blood leaks through a small tear in the inner wall, causing it to cut and dissect).
Consequences
The consequences for a patient with a ruptured brain aneurysm depend on the severity and location, the patient’s age, and his general and neurological health. Most patients (about 50%) with a ruptured brain aneurysm die from the initial bleeding. Another 20% die from complications and secondary stroke. Some patients recover almost completely without damage to the nervous system.
Early diagnosis and treatment are important in
preserving brain tissue from further damage.
Diagnosis of the disease
During diagnosis, obvious and additional symptoms of aneurysms are determined. The first category includes signs found in almost every patient:
- general weakness;
- blurred vision;
- fear of light;
- dizziness;
- nausea;
- hearing impairment;
- double vision;
- frequent headaches;
- numbness of the face and limbs.
Patients may also experience additional signs of pathology:
- noise in ears;
- dilation of the eye pupils;
- weakness in the legs;
- facial nerve paresis;
- drooping eyelid;
- twitching of the pupils.
Diagnosis of pathology is carried out using MRI or (the most effective method is still MRI). Modern diagnostic measures are able to determine the presence of an aneurysm in 98% of cases, including before its actual rupture. One of the most accurate methods for detecting pathology is subtraction angiography. It is necessary to carry out diagnostic measures when the above symptoms are detected.
What actions to take
Surgical intervention
Choosing the optimal surgical treatment for a ruptured brain aneurysm involves many factors, such as symptoms, size (aneurysms smaller than 3 mm do not need surgery), location and type of aneurysm (saccular aneurysms rarely rupture), and the patient's health and medical history.
There are 2 main treatment options for patients who require surgical removal of an aneurysm:
- Clipping;
- Endovascular therapy.
Clipping
Duration – 3-4 hours, takes place under general endotracheal anesthesia.
The operation is performed by a neurosurgeon who performs a craniotomy, isolates a vessel (or a set of arteries and vessels) with an aneurysm and places a clip on its isthmus. Clips (clamps) are made of titanium and are placed across the aneurysm. This prevents blood flow into the area of the aneurysm. Blood flow through the arteries is restored and the aneurysm is shut down. Most patients spend 2-3 nights in the hospital and then go home, with recovery lasting 1 to 2 months (with moderate activity restrictions).
Currently, neurosurgeons can perform a mini-craniotomy, or an incision just above the eyebrows, to perform clipping. A small incision above the eyebrow is made in the bone above the eye, through which a clip is “put on” the aneurysm. Such patients usually spend no more than 1-2 days in the hospital and then return home. They are practically unlimited in activity. Minicraniotomy is an invasive procedure and takes longer than endovascular surgery.
This operation is shown in the video
Endovascular intervention
Duration: 1.5-3 hours, takes place under general endotracheal anesthesia.
Endovascular surgery is performed by a neurointerventional surgeon. The prognosis for patients with a ruptured aneurysm who undergo endovascular surgery is better than after clipping. The procedure is performed using angiography. The catheter is inserted into the patient's vessel through the femoral artery; a special balloon (usually a platinum microcoil or microspiral) is placed at the end of the catheter. The coil is passed to the site where the aneurysm is located, forming an artificial clot that prevents blood flow and shuts off the aneurysm from the bloodstream. Most patients spend one night in the hospital and return to normal activities within 1-2 weeks.
Additional devices, such as a stent, may be needed to help place and maintain coils/coils at the site of the aneurysm. A stent is placed in a vessel adjacent to the aneurysm to provide support to the coil that holds the aneurysm sac in place and prevents blood flow.
Currently, surgeons are using embolization devices as a new technology. They are similar to stents in that they are placed in the main vessel adjacent to the aneurysm. These devices divert blood flow away from the aneurysm and allow the vessel wall to heal quickly. Over time, the aneurysm disappears.
This technology allows doctors to treat many aneurysms that were previously considered incurable.
Strengthening the walls of blood vessels
This method is used quite rarely. It involves wrapping a damaged vessel with an aneurysm with special gauze, which provokes the formation of an artificial blood clot (capsule) at the site of the aneurysm.
The consequences of hardening of the vessel walls
often include repeated heavy bleeding , and the symptoms of the disease may worsen.
Complications after surgery
Endovascular surgery has a lower risk of complications than clipping in the short term. But with endovascular intervention, there is a small chance that the patient will undergo a repeat identical operation to reduce the chances of aneurysm rupture. Approximately 1 in 5 patients require further treatment.
The time required for full recovery after endovascular intervention is shorter. Many patients recover within a few weeks, while recovery from clipping may take 1-2 months.
Endovascular surgery carries the following risks and complications (in addition to the usual risks after surgery):
- Bleeding around the graft;
- Bleeding before or after the procedure;
- Stent blockage;
- Nerve damage during surgery;
- Kidney failure;
- Decreased blood supply to the legs, kidneys or other organs;
- Erectile disfunction;
- Stent slippage.
Complications after clipping include:
- Breathing problems;
- Reaction to drugs;
- Brain swelling;
- infection in the brain or area around the brain;
- Stroke.
Open surgery can cause problems with speech, memory, muscle weakness, loss of balance, vision, coordination and other functions. Symptoms may be mild or severe.
Forecast
After successful surgery for a bleeding/ruptured aneurysm, the possibility of rebleeding is virtually eliminated. The prognosis also depends on whether there was brain damage from bleeding before, during, or after surgery.
Non-surgical methods
Drug therapy
Medicines that relieve symptoms may be used as first-line treatment for an unruptured aneurysm and to prevent it from rupturing:
- Calcium channel blockers - prevent spasms of the brain and blood vessels - Amlodipine Sandoz (indicated for arterial hypertension, to strengthen blood vessels, price for tablets 10 mg 30 pcs. 255 rubles), Zanidip-Recaordati (indicated for essential hypertension and for strengthening blood vessels, price for tablets 10 mg 28 pcs. 296 rubles);
- Painkillers - Nurofen (has an anti-inflammatory, analgesic effect, price for 200 mg tablets 8 pcs. 106 rubles); Flamax-Forte (for acute pain syndrome, price 100 mg 20 pcs. 132 rubles);
- Antiemetics – Zofran (to eliminate postoperative nausea/vomiting, price 4 mg 10 pcs. 2597 rubles); Latran (against nausea and vomiting, price 4 mg 10 pcs. 318 rubles);
- Drugs that stabilize blood pressure - Lorista (hypotensive drug, price 100 mg 30 pcs. 325 rubles); Corinfar Retard (hypotensive drug, reduces pressure on the walls of blood vessels, price 20 mg 30 pcs. 114 rubles);
- Anticonvulsants – Seduxen (sedative, anticonvulsant, price 20 mg 20 pcs. 15-60 rubles); Sibazon (sedative psychotropic drug, price 5 mg 20 pcs. 58 rubles).
All medications are prescribed by the attending physician.
Treatment
The purpose of such an operation is to turn off the aneurysm from the general blood flow, while maintaining the functionality of the artery. Performing surgery involves the following steps:
- Opening the skull (trepanation).
- Retraction of the meninges.
- Isolation of a vessel with a thinned wall.
- Clipping an aneurysm - attaching a special clip to the pedicle.
All manipulations are carried out using microsurgical equipment and a microscope.
Allows access to brain tissue without violating the integrity of the skull bones. A catheter with a balloon or coil is inserted through a large vessel (femoral, carotid artery). Under the control of computed tomography, the balloon is installed in the cavity of the aneurysmal sac.
It is also possible to perform electrocoagulation and artificial thrombosis of the aneurysm.
Not only is a cerebral aneurysm dangerous for the patient, the consequences after surgery can also be negative. Possible complications:
- Breakthrough of the dome with a spiral or balloon.
- Displacement of brain tissue.
- Infection through an open wound.
- Increased thrombus formation.
It is best to resort to endovascular surgery, as it involves the least tissue damage and the greatest efficiency.
Rehabilitation
The need for repeat clipping is 35% within the first 14 days after the first bleeding. Therefore, neurosurgeons prefer to perform open surgical or endovascular intervention immediately after diagnosing an aneurysm to reduce risks.
The recovery process (especially after clipping) is lengthy and may take several months or years to fully restore all brain functions.
The incisions heal within 6 weeks. After the operation, the patient is provided with a clear set of instructions and prescriptions. After endovascular surgery, the patient may be prescribed blood thinners, such as aspirin, and other medications to relieve pain symptoms (pain medications are indicated for 1-3 weeks). Return to full activity after aneurysm clipping or endovascular intervention depends on the patient's condition before and immediately after treatment. A physical therapy program is tailored to each individual patient. Moderate activity after discharge is encouraged.
What a patient may encounter if an aneurysm ruptures
The consequences of a ruptured aneurysm are the most severe. They are more difficult to treat and are accompanied by residual effects:
- difficulty moving, convulsions and involuntary movements;
- tingling, numbness, decreased sensitivity of different parts of the body;
- difficulty swallowing food;
- speech disorders;
- epileptic seizures;
- character changes, pronounced apathy or aggressiveness may appear;
- pain syndrome in different parts of the body;
- problems with bowel movements.
Prevention
In addition to quitting smoking, changing the following factors through a healthy lifestyle reduces the risk of developing an aneurysm again:
- Hypertension is regulated through diet (excluding fatty, fried, spicy foods), exercise and medications that reduce high blood pressure and tension/pressure on the walls of blood vessels;
- Poor nutrition with a deficient energy balance is a risk factor for heart disease and can lead to obesity. By adhering to a balanced diet, the patient can lower cholesterol levels and reduce the risk of developing atherosclerosis;
- Lack of exercise – activity and sports help lower blood pressure;
- Excess weight and obesity both cause the heart to pump more blood, which increases blood pressure. Excess fat tissue can increase or create inflammation in the body. The body mass index of a patient with an aneurysm should be no higher than 25.
Rules for preparing for the event
Preparation differs between elective and emergency patients. For planned patients, the following measures are performed:
- Hospitalization in a hospital;
- Conducting urine and blood tests (read about general and biochemical blood tests separately), coagulograms, examinations for HIV, syphilis, hepatitis B and C, fluorography;
- Consultations with a neurologist, anesthesiologist, neurosurgeon;
- Obtaining consent for surgical intervention and familiarization with possible risks and complications;
- Shaving hair from the area of skin through which the incision will be made;
- Removing nail polish.
The last meal is taken in the evening on the eve of the upcoming intervention.
For patients admitted urgently due to complications, the following minimum preparations are performed:
- Hospitalization;
- Taking blood for tests;
- CT or MRI of the skull (depending on the prevailing clinic, other parts of the body may be examined);
- Correction of vital functions (respiration, blood pressure);
- If necessary, tracheal intubation.