Definition
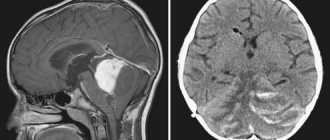
Arnold Chiari syndrome type I consists of the descent of the lower part of the cerebellum - the cerebellar tonsils - into the foramen magnum and spinal canal in the absence of other malformations associated with the spinal cord. Sometimes it is believed that the prolapse of the cerebellar tonsils should be more than 5 mm, sometimes more than 3 mm, for others the prolapse begins at 0 mm, when the tonsils are at the level of the border of the foramen magnum, in the presence of an appropriate clinical picture.
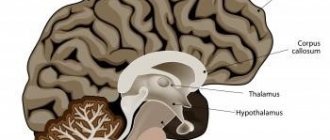
Figure 1.- The diagram shows the descent of the cerebellar tonsils and the increase in the supracerebellar space due to the displacement of the entire cerebellum towards the foramen magnum. Arnold Chiari I syndrome.
Description of the disease
For a long time it was believed that the anomaly was congenital, but it was found that it could also be acquired as a result of injuries, including birth injuries.
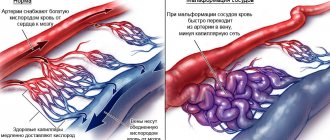
The essence of the disorder is anatomical deformation - incorrect (too low) location of the cerebellum and medulla oblongata. Their sections can extend from the posterior cranial fossa into the spinal canal, thereby disrupting the craniovertebral border - i.e. between the brain and spinal cord. This threatens to compress these areas of the brain and nerves and disrupt their functioning. The subarachnoid space, the cavity under the membranes of the brain through which cerebrospinal fluid moves, is also clogged. All this is dangerous due to neurological pathologies, cerebral hydrocephalus (hydrocephalus), stroke, and paralysis.
Symptoms
The clinical picture of Arnold Chiari I syndrome can be varied, the most common symptoms (from more frequent to rarer): headaches, pain in the cervical spine, paresis in the limbs, visual impairment, pain in the limbs, paresthesia, sensory disturbances, dizziness, swallowing disorders, lower back pain, memory impairment, gait disturbance, pain in the thoracic spine, imbalance, dysesthesia, difficulty expressing thoughts and finding words, sphincter disorders, insomnia, vomiting, loss of consciousness, trembling.
Diagnostics
The main diagnostic method for this pathology during the period of intrauterine development of the fetus is a screening ultrasound examination to identify developmental defects, but it does not give a 100% guarantee in this case.
Basic diagnostic procedures are carried out after the birth of the child . In the first year of life, this may be an ultrasound of the brain, until the large fontanel closes. In the future, patients with suspected such pathology undergo radiography of the skull and cervical spine for diagnostic purposes.
Based on the results of these studies, MRI diagnostics are performed; with maximum probability, it allows one to establish not only the final diagnosis, but also the degree of disorders and, in some cases, select adequate treatment.
Arnold Chiari types
There are 4 classical types (I, II, III, IV) and two recently described types (“0”, “1.5”):
Type I Prolapse of the cerebellar tonsils without any other malformation of the nervous system.
Type II Cerebellar tonsil prolapse with a neurovertebral malformation in which the spinal cord is attached to the spinal canal.
III type. Cerebellar tonsil prolapse with occipital encephalocele and cerebral abnormalities in Arnold Chiari II syndrome.
IV type. Dropping of the cerebellar tonsils, aplasia or hypoplasia of the cerebellum associated with aplasia of the tentorium.
“0” type Currently, cases of a clinical picture characteristic of Arnold Chiari Syndrome I, without prolapse of the cerebellar tonsils, have been reported.
“1.5” type. Recently, Arnold Chiari Syndrome 1.5 has been described with descent of the cerebellar tonsils and descent of the brain stem into the foramen magnum.
Risk factors
The risk of malformation in the fetus can be increased by factors such as:
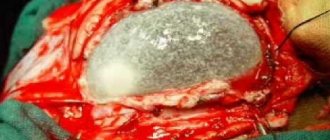
In this procedure, specially trained neurosurgeons remove bone and augment the brain padding—using the patient's own tissue in many institutions—to create excess space for cerebrospinal fluid and restore normal fluid circulation.
Although recovery from surgery can be challenging, most patients experience almost complete resolution of their symptoms. Our experienced medical team will develop a personalized treatment plan to help patients achieve the best results.
- Uncontrolled
use of medication during pregnancy; - Presence of
bad habits in a pregnant woman;
Infectious diseases suffered Such as rubella and others;- Problems
with proper nutrition in a pregnant woman.
Most experts are of the opinion that Arnold-Chiari syndrome
occurs against the background of genetic mutations in a child.
connection with the chromosomal abnormality has been found at this time .
The Chiari titanium pattern is sometimes associated with the development of syringomyelia, a fluid-filled cyst in the spinal cord. Arnold-Chiari deformity causes structural changes in the cerebellum and dislocations in the core. The cerebellum may be moved into the spinal canal of the upper spinal column. In some cases, there is also a brainstem dislocation originating from the cerebellum and spinal cord.
Causes of Arnold-Chiari malformation
The malformation was first described a century ago by the Austrian pathologist Hans von Chary. Arnold-Chiari lesions most often occur during prenatal development. The fetus has a very small posterior cavity in which the cerebellum does not fit and moves lower. The syndrome is associated with a problem with the flow of cerebrospinal fluid, or the fluid that surrounds the brain and protects it from shock. This obstruction causes hydrocephalic pathological accumulation of cerebrospinal fluid in the brain chambers. Arnold-Chiari syndrome can also be secondary to life, such as as a result of injury or infection.
Theories about the cause of cerebellar tonsil prolapse
Prolapse of the cerebellar tonsils can be the result of the tension that a particular malformation places on the spinal cord, with the exception of Arnold Chiari syndrome type I, in which prolapse of the cerebellar tonsils is the only disorder, and there are different theories about the cause of this disorder:
– Traditional theories:
- Hydrodynamic: prolapse of the cerebellar tonsils is a consequence of impaired circulation of the cerebrospinal fluid.
- Malformation: The theory about the small size of the foramen magnum, which provokes the descent of the tonsils into the spinal canal.
– The theory of spinal cord tension according to Filum System ®:
Dr. Miguel B. Royo Salvador's theory views the prolapse of the cerebellar tonsils in Arnold Chiari Syndrome I as a result of abnormal tension on the spinal cord due to an abnormal and tight ligament called the filum terminale. The terminal filament is not visible in the photographs.
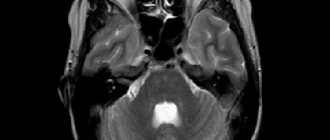
Figure 2. - MRI of the patient at 8 and 20 months, in the second image you can observe the prolapse of the cerebellar tonsils, which appeared after the first MRI. Huang P. “Adquired” Chiari I malformation. J. Neurosurg 1994. This indicates that, in addition to the hereditary and genetic factor, there is a factor of acquired disease.
Reasons for the anomaly
Scientists have not yet fully studied the causes of Arnold-Chiari syndrome
. Chiari malformation, as the anomaly is also called, can develop due to several factors.
Cervical and thoracolumbular syndrome. Although primarily empirical or occasionally anecdotal, several molecules have been used to treat this pathology with varying success. Although initial results after surgical therapy appear encouraging, especially in the short to medium term, further studies are needed to better determine effectiveness and determine the method of choice. From a preventive perspective, it is important that veterinarians, breeders and owners work together in selective breeding to minimize disease incidence.
Congenital:
- Incorrect development of the skull bones in the fetus
- too small a posterior fossa of the skull in a correctly developing baby leads to a discrepancy in the growth of the bones of the skull and brain. The cranial bones simply cannot keep up with the brain. - The fetus experiences a hyperincrease in the BZO.
Purchased:
- During childbirth, the baby
suffered a traumatic brain injury; - Due to impaired circulation
of livcore in the ventricles of the brain, damage to the spinal cord occurs. It thickens.
Arnold-Chiara syndrome can occur simultaneously or after other defects, for example, hydrocele of the spinal cord.
Tiama Tiari type 1 is a congenital abnormality of the cerebellum, the part of the brain located at the base of the skull. This causes pressure on surrounding tissue. If not treated properly, Chiari type 1 disease can affect almost all brain functions.
Other common symptoms may include diffuse numbness, tingling, pain or heaviness in the neck, torso, arms and legs. The list of less common symptoms is long and can include sensory and motor changes throughout the body. Both children and adults can experience.
- Difficulty swallowing.
- Difficulty breathing.
- Chiari falling into attack or short spells of fainting.
In children, boyish boys and boys manifest themselves in boys.
In adults, it is three times more common in women than men. Although the cause of Chiari disorder in children and adults is unknown, it is believed to begin in the early stages of brainstem and spinal cord development. In some cases, this is due to the lack of a typically small skull volume. Not so long ago, experts believed that this disease was congenital, but the percentage of patients with a congenital anomaly is much less than the percentage with an acquired one
syndrome.
Factors influencing the development of Arnold Chiari I Syndrome
The main factors involved in the development of Arnold Chiari Syndrome I are as follows:
- Family Predisposition: Tension of the nervous system due to an abnormally tight filum terminale, which we call filum terminale disease, leads to prolapse of the cerebellar tonsils. This pathology is genetic and can be inherited.
- Sudden increase in tension on the spinal cord: After a fall or spinal injury, existing tension on the spinal cord—filum terminale disease—may increase. In these cases, due to the stronger tension, the descent of the cerebellar tonsils or compression in the foramen magnum may increase, which will affect the growth of symptoms. Trauma, in this case, is not the cause of the development of Arnold Chiari syndrome, it is only a trigger for a sudden deterioration of the condition due to an increase in tension force.
Prevention of pathology
Due to the lack of sufficient information about the etiology of the disease, it is impossible to prescribe any preventive measures. All that can be done to prevent the development of the syndrome in the fetus is to carefully monitor the health of the mother . For this it is recommended:
- Stop taking alcohol, tobacco and drugs;
- Take care to create a balanced diet and exclude from it fried, salty and sweet foods, fast food, soda;
- Taking any medications, dietary supplements and vitamin complexes should only be taken under the supervision of a physician;
- Eliminate stress and groundless worries;
- Increase time spent outdoors;
- Regularly perform special physical exercises for pregnant women.
Complications of Arnold Chiari Syndrome I
Complications from prolapse of the cerebellar tonsils may depend on the degree of tension or on tissue compression in the occipital region (compression of the tissues of the cerebellar tonsils and the spinal cord stem due to limited space in the occipital space).
- Deterioration in quality of life: with Arnold Chiari I syndrome, headaches, dizziness, pain in the back and limbs, paresis, swallowing or sensitivity disorders, cognitive impairment, visual or gait disturbances can become chronic, increase in intensity, each time worsening the patient’s condition, limiting it normal lifestyle.
- Chronic pain: Patients may need treatment in a pain management unit because conventional anti-inflammatory and pain medications may not be effective in treating headache attacks and other symptoms.
- Sudden death: the spinal cord stem controls cardiorespiratory functions; if the cerebellar tonsils put pressure on it, breathing disorders (apnea, respiratory arrest, and even sudden death of the patient) may occur during sleep. That is why timely diagnosis and early treatment are so important.
Symptoms of the disease
Symptoms of Arnold Chiari disease can progress over several years. This is very dangerous, since there is a possibility of disruption in the functioning of the upper parts of the brain.
The appearance of symptoms and their severity depend on the type of disease and how severely the brain is affected. Most often, patients with this pathology present with the following complaints:
- The appearance of noise, hum or whistle when turning the head and at rest, which becomes louder over time;
- When you exercise, your head starts to hurt;
- Twitching of eyeballs;
- Increased intracranial pressure;
- Headache after sleep;
- Dizziness;
- Disorientation and clumsiness;
- Trembling of the hands and feet in the presence of a severe form of the disease;
- Deterioration of vision, appearance of fog before the eyes;
- Muscle weakness and numbness;
- Loss of sensation in half of the body or face;
- Loss of consciousness with sudden movements of the head, especially when turning;
- Decreased sensitivity of the limbs.
All symptoms usually worsen with turning the head and sudden movements. Complications of the disease include:
- Blindness;
- Complete or partial paralysis;
- Hydrocephalus;
- Syringomyelia;
- Spinal or cerebral infarction;
- Urinary incontinence;
- Apnea up to death.
Treatment of Arnold Chiari Syndrome I
Typically, neurosurgical treatment is used for Arnold Chiari Syndrome I with/without syringomyelia. Currently, decompression or craniotomy of the foramen magnum is the standard treatment for this diagnosis in most medical centers in the world. It is usually prescribed in cases where the symptoms cause more damage and mortality than the natural progression of the pathology.
However, since 1993, after the publication of the doctoral dissertation of Dr. Royo Salvador, who linked the tension of the entire nervous system with the filum terminale, the tension of which provokes, among other diseases, the prolapse of the cerebellar tonsils, a new treatment was developed, etiological, that is, eliminating the cause of the disease with surgical dissection of the filum terminale, which removes the pathological tension mechanism.
Our technique of filum terminale dissection is minimally invasive and is prescribed in all cases of filum terminale disease, both symptomatic and asymptomatic, and as early as possible, since the risks are minimal and much lower than from the pathology itself, in addition, this treatment stops further development of the disease.
Cutting the filum terminale with the Filum System® technique:
Advantages
1. Eliminates the cause of Arnold Chiari Syndrome I and associated pathologies.
2. Eliminates pressure in the foramen magnum and with it the risk of sudden death.
3. 0% mortality, without consequences in more than 1500 patients operated on using the Filum System® method.
4. With minimally invasive technique, surgical time: 45 minutes. Short stay in the clinic. Local anesthesia. Short period of post-operative recovery without restrictions.
5. Improves symptoms, stops the prolapse of the cerebellar tonsils.
6. Eliminates the risk of hydrocephalus due to prolapse of the tonsils.
7. Improves blood supply to the entire nervous system and, at the same time, cognitive capabilities, which may suffer due to spinal cord tension.
Flaws
1. A small suture in the coccyx area; complications such as suture infection and hematoma in the operation area are possible.
2. Improvement in spasticity is sometimes mistaken for decreased strength in the limbs.
3. During the process of restoration and improvement of sensitivity, unpleasant sensations may appear, which are usually mistaken for undesirable consequences.
4. With improved blood supply to the brain, brain activity may increase and mood swings may occur during the initial post-operative period.
Occipital craniectomy:
(Decompression of the foramen magnum)
Advantages
1. Avoiding the risk of sudden death.
2. The condition of some patients improves.
Flaws
1. Does not eliminate the cause of the disease.
2. Mortality from 0.7 to 12%, a higher percentage than sudden death with spontaneous development of the disease.
3. Aggressive surgery, crippling and possible consequences.
4. Small percentage of improvement and for a short period of time.
5. Neurological deficit: depends on the location of the injury: Emiparesia (paralysis of half the body from 0.5 to 2.1%. Changes in visual space from 0.2 to 1.4%. Changes in speech from 0.4 to 1%. Lack of sensitivity from 0.3 to 1%. Lack of balance, difficulty walking from 10 to 30%.
6. Postoperative intracerebral hemorrhage in the operated area, epidural hematoma, intra-axial hemorrhage, which can cause neurological deficit or worsening of a pre-existing deficit (0.1 to 5%).
7. Brain edema, depending on the process and situation, the risk reaches 5%.
8. Superficial, deep or intracranial infection, risk from 0.1 to 6.8%, with the formation of a brain abscess, aseptic-septic meningitis.
9. Hemodynamic changes due to manipulation of brain stem disorders.
10. Gas embolism (in patients in a sitting position).
11. Cerebrospinal fluid output is from 3 to 14% (cerebrospinal fluid fistula).
12. Postoperative hydrocephalus.
13. Pneumoencephaly
14. Tetraparesis (loss of strength in all limbs)
Due to the morbidity and mortality associated with occipital decompression, which exceeds the mortality associated with spontaneous development of Arnold Chiari I syndrome, we believe that this treatment is contraindicated.
Treatment Options
If the anomaly is asymptomatic (usually type 1), the patient does not require treatment. Nothing bothers him. However, if a violation of the location of the cerebellum is discovered by chance, it is necessary to be observed by a specialist. If complaints are limited to minor headaches, treatment is carried out conservatively. Conservative treatment is selected taking into account the symptoms. The following may be prescribed in various combinations:
- for dropsy - dehydration agents, most often (Diacarb, Veroshpiron),
- to combat headaches - non-steroidal anti-inflammatory drugs (Diclofenac, Ibuprofen, Ketanov, Nimesulide and others),
- to maintain muscle functions - various muscle relaxants,
- against dizziness - vestibulocorrectors.
To improve metabolic processes in nerve tissues and combat the lack of oxygen in them, all patients are recommended to take:
- neuroprotectors (Cerakson, Farmakson),
- vascular agents (Cytoflavin, Nicotinic acid),
- metabolites (Cerebrolysin, Cortexin),
- antioxidants (Mexiprim, Mexidol),
- B vitamins (Milgamma, Combilipen).
Often, for patients with type 1 Arnold-Chiari malformation, conservative treatment is quite sufficient to correct the clinical picture of the disease.
Surgery is usually performed in more severe cases. If the 1st type of malformation does not always require treatment, then the second requires surgical intervention as quickly as possible. The operation is prescribed for all patients in childhood. It is impossible to delay surgical treatment, since it gives a chance to restore speech and motor functions, sensitivity and normal functioning of the central nervous system as a whole.
Surgery is also performed if drug therapy has no effect.
The operation may be a bypass. Using a shunt, excess cerebrospinal fluid (CSF) that accumulates in the skull is removed. Another type of operation is trephination and modification of the bones of the back of the skull with the removal of sections of the cerebellum protruding downward. At the same time, excision of adhesions and cysts existing in the subarachnoid space, which interfere with the free flow of cerebrospinal fluid, is performed.
After surgical treatment, the patient must undergo a long period of rehabilitation. In many cases, a person becomes disabled. Even if disability is avoided, residual neurological consequences may continue to occur. Young men with this disease are usually considered unfit or partially fit for military service.
BIBLIOGRAFIA
- Dr. Miguel B. Royo Salvador (1996), Siringomielia , escoliosis y malformación de Arnold-Chiari idiopáticas, etiología común (PDF). REV NEUROL (Barc); 24 (132): 937-959.
- Dr. Miguel B. Royo Salvador (1996), Platibasia , impresión basilar, retroceso odontoideo y kinking del tronco cerebral, etiología común con la siringomielia , escoliosis y malformación de Arnold-Chiari idiopáticas (PDF). REV NEUROL (Barc); 24 (134): 1241-1250
- Dr. Miguel B. Royo Salvador (1997), Nuevo tratamiento quirúrgico para la siringomielia , la escoliosis , la malformación de Arnold-Chiari , el kinking del tronco cerebral, el retroceso odontoideo, la impresión basilar y la platibasia idiopáticas (PDF). REV NEUROL; 25 (140): 523-530
- M. B. Royo-Salvador, J. Solé-Llenas, J. M. Doménech, and R. González-Adrio, (2005) “Results of the section of the filum terminale in 20 patients with syringomyelia , scoliosis and Chiari malformation .” (PDF). Acta Neurochir (Wien) 147:515–523.
- M. B. Royo-Salvador (2014), “Filum System® Bibliography” (PDF).
- MB Royo-Salvador (2014), “A Brief Introduction to the Filum System®.”
Arnold Chiari syndrome I
Described: In 1883 by the anatomist surgeon John Cleland (1835-1925) from Perthshire, Scotland.
He described elongation of the cerebellar vermis, prolapse of the cerebellum and fourth ventricle in a boy with hydrocephalus, encephalosceles, and spina bifida. In 1891 and 1896, Hans Chiari described new cases and classified them. In 1894, Jules Arnold contributed to the spread of knowledge about this disease. Named: Schwalbe and Gredig in 1907 as “Arnold-Chiari malformation.” The official modern nomenclature in the codification and classification of diseases of the World Health Organization calls this disease the term “Arnold-Chiari syndrome or disease I” (Q07.0, CIE-10). (WHO, (International Statistical Classification of Diseases and Related Health Problems, 10th Revision (c) Geneva, OMS, 1992)).
Frequency: One case per thousand newborns, other authors indicate less than 1% of the population. In both cases, we are talking about prolapse of the cerebellar tonsils by more than 3 or 5 mm.
Treatment
Dystopia of the cerebellar tonsils has two methods of treatment - surgical and non-surgical (conservative). If the anomaly occurs without symptoms, then treatment is not necessary. If the syndrome manifests itself only as pain in the neck and back of the head, then conservative therapy should be carried out. The patient is prescribed anti-inflammatory and painkillers.
When conservative treatment does not help get rid of symptoms, surgery is prescribed. The purpose of surgery is to eliminate factors that exert pressure and compress the structures of the brain. After the procedure, the occipital part of the head should expand, which will improve and normalize the movement of cerebrospinal fluid within the body. There are options for bypass surgery.
Filum terminale disease
After the research of Dr. Royo Salvador and his doctoral dissertation (1992), it was found that several diseases whose cause was previously unknown, such as: Arnold Chiari I syndrome, idiopathic Syringomyelia and Scoliosis, Platybasia, Basilar Impression, Axial vertebral tooth displacement, An angular bend at the level of the arch of the atlas is part of a new pathology - Diseases of the filum terminale - and arises for the same reason: tension in the spinal cord and the entire nervous system.
The tension force of the entire nervous system during filum terminale disease is present during the formation of all human embryos; to a greater or lesser extent, everyone suffers from its consequences and various forms of manifestation and intensity.
The following diseases may be associated with filum terminale disease: intervertebral hernias, some cerebrovascular insufficiency syndromes, facet syndrome, Bostrup syndrome, fibromyalgia, chronic fatigue, nocturnal enuresis, urinary incontinence and acute paraparesis.
For accurate diagnosis, selection of treatment and monitoring of a patient with filum terminale disease, the Filum System® method was created.
Causes
The exact causes of Arnold-Chiari malformation have not been established at the moment. Doctors identify the following factors that may increase the risk of developing pathology:
- the brain has increased in size;
- the cranial fossa has decreased;
- smoking, alcohol during pregnancy, which caused fetal intoxication.
Arnold-Kari anomaly can be a consequence of improper planning and management of pregnancy. Alcohol intoxication, excess medications, viral diseases, smoking are the most dangerous risk factors that can cause a variety of defects in the fetus. According to another version, the anomaly becomes a consequence of a violation of the development of the skull. The progression of the pathology can be caused by traumatic brain injuries and hydrocephalus.