Drum string
(Chorda tympani) - a thin branch originating from the 7th pair of cranial nerves (N. facialis), which passes through the tympanic cavity above the tendon of the muscle that stretches the tympanic membrane, exits the tympanic cavity and connects through the so-called Glaser's fissure (Fissura Glaseri) a branch with the ganglion oticum, then merges with the lingual nerve (one of the branches of the third branch of the trigeminal nerve) and together with it enters the hypoglossal ganglion and tongue. Chorda tympani leads excretory and vasodilator fibers to the submandibular and sublingual salivary glands. Its irritation causes the submandibular gland to overflow with blood with copious secretion of very liquid saliva (as opposed to the separation caused by irritation of the sympathetic nerve).
Facial nerve damage
The facial nerve also supplies the laryngeal supersili and the procurus, both of which make a second contribution to the retraction of the upper eyelid. Sympathetic fibers promote retraction of the upper eyelids by innervating the superior muscle, also known as Müller's muscle.
What tests and diagnostics do you need to undergo for the facial nerve?
Sympathetic fibers also innervate the inferior palmar muscle, which helps reduce inferior return. The terminal branches of the ophthalmic trim supply the upper eyelid as the lacrimal, supraorbital, and supratrochlear nerves, and the medial aspect of both the superior and inferior lids as the infratrochlear nerve. The terminal branches of the maxilla subdivide the lower eyelid, as do the zygomatic facial and infraorbital nerves.
Encyclopedic Dictionary F.A. Brockhaus and I.A. Efron. - St. Petersburg: Brockhaus-Efron. 1890-1907.
See what “Drum string” is in other dictionaries:
- Drum string
- a system of nerve fibers that forms a portion of nerve fibers of the 4th pair of cranial nerve. Carries some part of taste information. Since the drum string passes through the middle ear, it is open to experimentation...
The facial nerve supplies the lateral inferior lid, and the infraorbital nerve supplies the lower eyelid. In addition to innervating the levator pallis suprarior, somatomotor fibers of the oculomotor nerve also supply the medial, superior and inferior rectus muscles and the inferior oblique muscles. The oculomotor nerve also carries parasympathetic fibers that supply the intrinsic muscles of the eye and transmits opreception from the extraocular muscles.
Its bundles combine with other somatomotor and parasympathetic divisions to form the oculomotor nerve, which emerges from the brainstem between the posterior cerebral and superior cerebellar arteries. After exiting the brainstem, the oculomotor nerve courses medially and gives way to the edge of the tentorium before entering the roof of the cavernous sinus. In the cavernous sinus, the oculomotor nerve travels along the lateral wall and receives sympathetic fibers from the plexus of the internal carotid artery. The nerve then exits the skull through the superior orbital fissure through the oculomotor foramen and divides into superior and inferior divisions.
DRUM STRING
- A system of nerve fibers that forms part of the IV cranial nerve. It carries part of the nervous information from taste buds and, since it passes through the middle ear, where it is available for experiments, plays an important role in obtaining information... ... Dictionary of Psychology
The superior division passes into the orbit medially to the optic nerve and is inferior to the superior rectus muscle. It then divides into several bundles of fibers which pass or move medially into the superior rectum, finally inserting onto the inferior surface of the leptera palmaris.
Which doctors should I contact to examine the facial nerve?
The inferior division of the oculomotor nerve moves inferiorly to supply the medial rectus, inferior rectus, and inferior oblique muscles. The lower section also contains autonomic fibers intended for the ciliary ganglion and the internal muscles of the eye. Sensation to the eyelids is provided by the terminal branches of the ophthalmic and maxillary divisions of the trigeminal nerve. The cell bodies of the terminal branches originate from the trigeminal ganglion.
String: Wiktionary has an entry for “string” String (music) part of stringed musical instruments, the primary source of sound ... Wikipedia
Cord tympani neuralgia
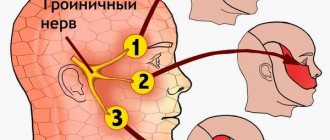
— The chorda tympani provides sensitivity to the structures of the middle ear, auditory tube, mastoid process, and taste sensitivity to the anterior 2/3 of the tongue. Its neuralgia is manifested by paroxysms of intense, shooting pain in the ear. Described in 1908 ... Encyclopedic Dictionary of Psychology and Pedagogy
The ophthalmic division arises from the anterior aspect of the trigeminal ganglion, and its sensory supply to the eyelid ends as the lacrimal, supraorbital, and supractriclar nerves supplying the upper eyelid, and the infratochlear nerve supplying the medial upper and lower eyelids. As it passes through the cavernous sinus, it receives sympathetic fibers from the plexus of the internal carotid artery and divides into lacrimal, frontal and nasociliary nerves. The lacrimal nerve enters the orbit through the superior orbital fissure, courses along the superior border of the lateral rectus muscle, and enters the lacrimal gland. Part of the lacrimal nerve terminates in the lacrimal gland, but some fibers pass through or around the gland to innervate the conjunctiva and lateral skin of the upper eyelid. The supraorbital nerve travels along the orbital midline and emerges superomerno with the supraorbital artery to supply the conjunctiva and skin of the central two-thirds of the upper eyelid. The supraorbital nerve provides additional sensation to the forehead and scalp. The lateral branches of the supraorbital nerve move in the muscular fascia deep to the facial muscles in the forehead, but become superficial at the level of the scalp. The medial branches of the supraorbital nerve pass through the facial muscles more proximally and move superficially to the forehead and scalp. The nasociliary nerve enters the orbit through the superior orbital fissure and moves laterally to the optic nerve. It gives off sensory branches to the ciliary ganglion, crosses the optic nerve medially, and gives off long ciliary branches. The nasociliary nerve then branches off sensory branches to the reticular sinus and continues to run along the superior border of the medial relaxator muscle as the infartrochlear nerve. It emerges from the orbit over the medial canthal tendon and supplies the medial structures of the external eye, including the medial conjunctiva, caruncle, lacrimal sac, and medial upper and lower eyelids. The maxillary division arises from the posterolateral aspect of the trigeminal ganglion, and its sensory supply to the eyelid ends as the zygomatic physiological nerve supplying the lateral lower eyelid and the infraorbital nerve supplying the lower eyelid.
- (aurus media) part of the ear between the outer and inner ear, performing a sound-conducting function. The middle ear is located in the temporal bone and consists of three interconnected air cavities. The main cavity is the tympanic cavity (cavum... ... Medical encyclopedia
- (nervi craniales; synonym cranial nerves) nerves extending from or entering the brain. There are 12 pairs of Ch. n., which innervate the skin, muscles, glands (tear and salivary) and other organs of the head and neck, as well as a number of organs... ... Medical encyclopedia
It then enters the lizard pterygopalatine and secretes the palatine branches, nasal branches and the zygomatic nerve. The terminal branch enters the orbit through the inferior orbital fissure as the infraorbital nerve. The intraorbital nerve runs along the orbital floor with the sculomic nerve in the infraorbital groove. The infraorbital nerve then enters the infraorbital canal and exits the orbit through the infraorbital foramina with the infraorbital artery. After emerging, the infraorbital nerve forms the external nasal, internal nasal, labial and palpebral branches.
Facial nerve ... Wikipedia
Temporal bone
— The temporal bone, os temporale, steam room, is involved in the formation of the base of the skull and the lateral wall of its vault. It contains the organ of hearing and balance. It articulates with the lower jaw and is the support of the masticatory apparatus. On the outer surface ... Atlas of Human Anatomy
The palpebral branch innervates the lower eyelid and conjunction through medial and lateral branches. Before exiting the orbit, the zygomatic nerve divides. It forms the zygomaticotemoporal and zygomaticofacial nerves. The zygomaticomembranous nerve exits the orbit through the zygmaticotemporal foramen and supplies the skin of the lateral temple. The marsh physiological nerve exits the orbit through the zygomatic canal and supplies the lateral cheek and lateral lower eyelid.
Motor neurons originate in the pons. The motor division then enters the internal auditory canal, passes through the ganglion ganglion, moves adjacent to the mastoid cells, and exits the skull through the stylomastoid foramen. After emerging from the stylomasoidal foramen, the facial nerve ascends into the parotid gland, crosses the external carotid artery, and divides into the superior temporomandibular and inferior cervicofacial divisions. The temporal and zygomatic rami supply the frontalis and facial muscles on their deep surfaces.
MIDDLE EAR
- MIDDLE EAR. Phylogenesis. In the historical development of the hearing aid, at a certain stage the auxiliary, so-called inner ear begins to join the more ancient formation of the inner ear. sound-conducting section, the deeper part of the horn is C...
The temporal branch becomes superficial as it moves toward the lateral orbit and innervates additional facial muscles. The buccal branch may provide additional innervation to the eyelid muscles; the superficial branch of the buccal runs medially and is excellent to supply the superomedial tunica, procura and corrugators. Sympathetic supply to the muscles of the eyelids occurs in the hypothalamus. Hypothalamic neurons pass ipsilaterally to the brainstem and synapse in the spinal cord. Second order neurons exit the spinal cord, travel along the sympathetic chain and synapse in the superior cervical ganglion.
HUMAN NERVES
— HUMAN NERVES. [Anatomy, physiology and pathology of the nerve, see art. Nerves in Volume XX; in the same place (Art. 667 782) drawings of Human Nerves]. Below is a table of nerves, highlighting in systematic order the most important points of the anatomy and physiology of each... ... Big Medical Encyclopedia
Facial nerve lesions
Third-order neurons then travel along the carotid artery, follow the internal carotid artery, and enter the cavernous sinus. From here, the fibers most likely project from the internal carotid artery to the ophthalmic division of the trigeminal nerve and enter the orbit through the superior orbital fissure to supply the superior and inferior muscles. However, the exact route of sympathetic fibers distal to the cavernous sinus remains controversial.
See what “Drum string” is in other dictionaries
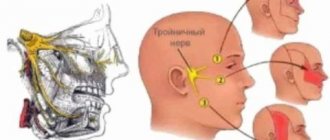
The nerves distributed throughout the face are branches of the facial nerve. These are the temporal, zygomatic, buccal, marginal, mandibular and cervical branches. The character of the facial nerves changes. The trigeminal, or fifth cranial nerve, provides sensory input to the skin of most of the face, with the exception of some parts of the skin around the ear and the angle of the jaw.
The topographic anatomy of the facial nerve is quite confusing, due to the fact that it passes through the facial nerve, receiving and giving off processes.
Where does it start?
It arises from three nuclei at once: motor, secretory and sensory fibers. Then through the auditory opening it passes into the thickness of the temporal bone into the internal auditory canal. Here the intermediate nerve is added to it, and a knee is formed at the bend of the canal, which, taking the form of a node, gives the intermediate nerve the property of sensitivity. The anatomy of the facial nerve and its diagram will be discussed in this article.
Marginal mandibular branch of the facial nerve
Lymphatics of the face and scalp are simple. Use caution when performing facial acupuncture to avoid bruising, which can damage the face or trigeminal nerve, causing facial weakness or excessive sensitivity. As the upper neck flap is elevated, attention should be paid to preserving the marginal mandibular facial nerve. Injury to this nerve causes obvious cosmetic deformity with asymmetry in the movement of the angle of the mouth. It may also contribute to drooling and difficulty swallowing due to the inability to maintain labial closure during the preparatory phase.
Features of the pathology
The nerve ganglion of the ear has a complex structure, which is formed by sensory and autonomic nerve fibers. With neuralgia of the ear, people note the following symptoms:
- excessive salivation;
- sharp and shooting pain in the ear;
- feeling of stuffiness in the ear.
Often the pain is reflected in the lower jaw, which makes it difficult to identify the cause of the pain syndrome and make a diagnosis, which requires consultation with three specialists - a dentist, an otolaryngologist and a neurologist.
Division into processes
To enter the thickness of the parotid gland, the facial nerve is divided into separate processes: the lingual branch, the posterior auricular nerve, the digastric and stylohyoid branches. The intermediate gives off branches such as the stapedius and petrosal nerves, connective tissue with the tympanic weave and the vagus nerve, and the terminal branch (corda tympani). The anatomy of the facial nerve is unique.
Topography of the crow's foot
If it is not immediately visible, the nerve can be located by careful dissection.
Nerve stimulator use should be minimized with power at its lowest setting, as repeated stimulation of the nerve may result in neurapraxia. It is located lower on the submandibular gland. Once both branches have been identified, the cervical spine may need to be sacrificed; this can be done without permanent functional deficit. Note that since the platysma muscle contributes to the downward movement of the lower lip, any anterolateral incision through the platysma will cause some degree of disruption of lip movement. The approach to preserving this nerve varies depending on the presence or suspicion of pathological lymph nodes along the external facial vein. When such nodes are likely, the nerve should be preserved by identifying it as it passes through the vein and carefully dissecting it without surrounding tissue, which should be included in the surgical specimen.
Symptoms
The great auricular nerve has a very important job. With neuralgia of the ear, pain can be transmitted to the jaw, but patients more often report pain in the ear and around its shell, extending to the temporal zone. The pain occurs in the form of attacks, and may worsen under certain influences. Factors that increase this pain include eating hot food, humid weather, stress or emotional tension.
Attacks of pain are short-lived and can last from a couple of minutes to one hour.
Branches
Once again, the facial nerve diverges in the thickness of the parotid gland, giving two main branches - a small lower and powerful upper, which then also branch, moreover, radially: up, forward and down to the facial muscles. As a result, the parotid plexus is formed.
The facial nerve (the anatomy diagram will be presented in the photo) consists of the following parts:
If a nerve must be mobilized to preserve it, the technique used during dissection should avoid trauma to the nerve through direct contact with instruments or elevate and stretch the nerve as much as possible. The mobilized nerve can then be protected during further dissection by securing the perineural tissue to an elevated superior skin flap.
The outer facial vein is also ligated inferiorly as it emerges from the fatty tissue in the submandibular triangle, and the superior stump of the vein is removed with a skin flap. This can be done with magnification using an 8-0 to 10-0 niobile suture placed in the epineurium.
- nerve trunk (more precisely, its processes);
- the spaces of the cerebral cortex, which are responsible for the work of facial muscles;
- nuclei located between the bridge and the medulla oblongata;
- lymph nodes and a network of capillaries that feed nerve cells.
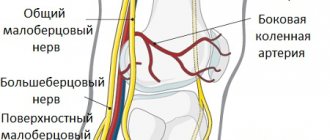
Cervical and brachial plexuses, their formation by spinal nerves. Innervation area
Maksimenkova, L., 1963; Multi-volume guide to neurology, ed. S. N. Da-videnkova, vol. 3, book. 1, p. 99, M., 1962; GG about pel I N with to and J1 Ya. Yu. Vertebrogenic diseases of the nervous system, vol. 3, Kazan, 1981, bibliogr.; Ratner A. Yu. and Soldatova L. P. Obstetric paralysis in children, Kazan, 1975; Sinelnikov R.D. Atlas of human anatomy, vol. 3, p. 24, M., 1981; Triumphov A.V. Topical diagnosis of diseases of the nervous system, L., 1974; Favorsky B.
A. On the issue of intra-stem architectonics of the peripheral nervous system, Zhurn. neuropath, and psychiatrist., t. 61, no. 2, p. 305, 1961; Clara M. Das Nervensystem des Menschen, Lpz., 1959.
I. P. Antonov (pathology), V. I. Kozlov
(an.).
Functions
Anatomy (diagram posted above) is discussed. Now let's talk about its functions.
The main task of the facial nerve is to provide motor functions of the face. However, everything is complicated by the fact that before it branches into small parts, it is intertwined with the intermediate nerve and partially shares responsibilities with it. Through the internal auditory opening they move into the tunnel of the facial nerve, where it forms a genu that provides sensory input to the intermediate nerve.
The facial nerve underlies the motor activity of almost all facial muscles, but in combination with the intermediate nerve it possesses taste and secretory fibers.
The pattern of the fibers of the facial nerve is very interesting and requires careful consideration.
Supraclavicular part of the brachial plexus
The supraclavicular part, pars supraclavicularis , of the brachial plexus (see Fig. 1007, 1010) gives nerves to the deep muscles of the neck, some muscles of the upper limb girdle, back and chest.
These first include muscle branches, the dorsal nerve of the scapula, the long thoracic nerve, the subclavian nerve, and the suprascapular nerve.
1. Muscular branches are short nerves that go to the deep muscles of the neck.
They depart from the branches of the plexus immediately after they emerge from the intervertebral foramina and are directed to the intertransverse muscles, the anterior, middle and posterior scalenus, and the longus colli muscle.
2. Dorsal nerve of the scapula, n. dorsalis scapulae (CV) (see Fig. 1007), originates from the posterior part of the infraclavicular part of the plexus, follows the anterior surface of the levator scapulae muscle, between it and the posterior scalene muscle, and goes to the medial edge of the scapula.
Here it gives branches to the rhomboid major and minor muscles and to the lower parts of the levator scapulae muscle.
3. Long thoracic nerve, n. thoracicus longus (CV–CVII), CVIII (see Fig. 1007, 1010), is directed down along the anterior axillary line along the lateral surface of the serratus anterior muscle and enters with its branches into the thickness of its teeth.
4. Subclavian nerve, n. subclavius (CIV–CVI) (see Fig. 1007), is a thin nerve, located in front of the subclavian artery, lateral to the lower part of the anterior scalene muscle, and follows the subclavian muscle.
It often gives off a connecting branch to the phrenic nerve, which approaches the latter from its lateral side.
Rice. 1013.
Facial nerve lesions
If the canal is malfunctioned or infringed, paralysis of the motor muscles of the face may occur. Its asymmetry is visually observed: the relaxed part has a mask effect due to its immobility, the eye on the affected side does not close, and lacrimation increases due to the fact that the mucous membrane is irritated by dust and air, which, in turn, can cause conjunctivitis. Wrinkles on the forehead and the area around the nose and lips are straightened, the corners of the mouth are directed downward, the person cannot wrinkle his forehead.
In humans, the facial nerve is often affected (its branches, their anatomy and topography are presented in detail in the photo).
If for any reason the main motor function is affected, then we are talking about peripheral paralysis. It is characterized by the following external signs: paralysis of the muscles responsible for facial expressions, complete asymmetry of the face, the speech apparatus is impaired, fluid intake can be limited. If the nerve was affected at a time when it was located in the pyramidal bone, then in addition to the signs listed above, deafness and lack of taste are also noted.
Neuritis is a neurological disease characterized by an inflammatory process. It can appear in the central part of the face and in the periphery. Symptoms depend on the area of the nerve affected. The disease develops either due to hypothermia (primary neuritis) or as a complication of other diseases (secondary).
It is characterized by an acute onset, the pain radiates behind the ear, and after a few days facial asymmetry is observed. Symptoms may vary depending on the part affected. When the nucleus of the facial nerve is damaged, a person develops muscle weakness of the face. When a nerve is pinched in the area of the pons of the brain, strabismus occurs, as well as paralysis of almost all the facial muscles. If the infringement occurs at the exit, it will result in impaired or short-term hearing loss. The human facial nerve is important. The structure, functions and problems have been studied for a long time.
In chronic otitis media, neuritis may be concomitant, arising due to inflammation in the middle ear, and therefore may be accompanied by a sensation of lumbago. If accompanied by mumps, then symptoms of general intoxication appear - chills, body aches, high fever.
What to remember?
For neuralgia of the ear, it is impossible to use traditional healing technologies based on exposure to heat. In this case, heating can provoke the progression of the inflammatory process. If ear pain occurs suddenly, and there is no general malaise or symptoms of a cold, you should first consult a neurologist.
If discomfort is accompanied by an increase in temperature, you need to go to an appointment with an otolaryngologist. Often neuralgia becomes the patient’s constant companion. Due to the fact that the pain does not go away on its own, and the attacks do not last long, people prefer to ignore the discomfort. This approach is incorrect, because any illness should be treated in a timely manner.
Principles of therapy
The treatment regimen for the facial nerve for pinching and inflammatory processes must necessarily be comprehensive. Therapy includes:
- diuretics, which remove fluid from the capillary network;
- glucocorticosteroids;
- drugs that dilate blood vessels;
- vitamins (usually group B).
Such treatment eliminates the main cause of the disease, since inflammation of the facial nerve is often the result of another disease, a secondary disease. Nervous illnesses are most often accompanied by very unpleasant sensations, so the patient is prescribed analgesic drugs. For treatment to be faster and more effective, the facial muscles need to be provided with complete rest.
The complex treatment also includes physiotherapeutic procedures. From the second week of the disease, it is allowed to use facial massage and engage in physical therapy with a gradually increasing load. Surgery is very rarely required. Surgical treatment is indicated when neuralgia is congenital or occurs after a mechanical injury. An operation of this kind consists in stitching together improperly fused and torn nerve endings. Also, surgical intervention is legal if drug treatment is ineffective for six months (maximum eight months). If you ignore the process and do not use the listed methods of therapy, the facial muscles can completely atrophy without the possibility of recovery in the future. The only way out is surgical facial plastic surgery, the material for which is taken from the victim’s leg.
Causes
As a rule, neuralgia of the ear node develops due to the presence of a source of infection in the body. Viruses spread through the bloodstream throughout the body and enter the area of the cranial nerves, activating inflammation. Neuralgia can be caused by:
- blockage or inflammation of the salivary glands;
- sinusitis;
- sore throat, including prolonged ones;
- purulent and prolonged inflammation of the middle ear (otitis);
- infectious and bacterial dental diseases.
Sometimes secondary inflammation of the greater auricular nerve is detected. This occurs in diseases such as sepsis, pneumonia and kidney pathologies. Damage to the auricular ganglion may be one of the manifestations of diabetic polyneuropathy.
Research methodology[edit | edit code]
When starting an examination of the patient, it is first necessary to note the presence or absence of disturbances in facial expressions and movements of facial muscles.
When the facial nerve is damaged, the natural folds on the forehead and nasolabial folds are smoothed out. Pay attention to the width of the palpebral fissure, the location of the eyebrows, etc.
The patient is asked to perform a series of tests:
- close eyes
- close alternately first one and then the other eye
- close your eyes
- raise your eyebrows
- frown
- wrinkle your nose
- bare your teeth
- puff out your cheeks
- blow, whistle
- form a crease in the neck
You should make sure that the movements are performed equally on both sides.
It is also necessary to check the patient's taste sensitivity on the anterior 2/3 of the tongue.