| Nervus vagus | |
| Superior parts of the glossopharyngeal nerve, vagus and accessory nerves | |
| Direction of the glossopharyngeal nerve, vagus and accessory | |
| Latin name | nervus vagus |
| Innervation | levator velum palati muscle, tubopharyngeal, palatoglossus and velopharyngeal muscles, superior, middle and inferior pharyngeal constrictors |
| Begins | medulla |
| Catalogs |
|
Nervus vagus
(lat. nervus vagus) - the tenth pair of cranial nerves (X pair), paired nerve. Goes from the brain to the abdominal cavity. Innervates the organs of the head, neck, chest and abdominal cavities.
It is mixed - contains motor, sensory and autonomic (sympathetic and parasympathetic) fibers [1]. Provides:
- motor innervation of the muscles of the soft palate, pharynx, larynx, as well as striated muscles of the esophagus
- parasympathetic innervation of the smooth muscles of the lungs, esophagus, stomach and intestines (up to the splenic flexure of the colon), as well as the muscles of the heart. Also affects the secretion of the glands of the stomach and pancreas
- sensitive innervation of the mucous membrane of the lower part of the pharynx and larynx, the skin behind the ear and part of the external auditory canal, the eardrum and the dura mater of the posterior cranial fossa.
Anatomy
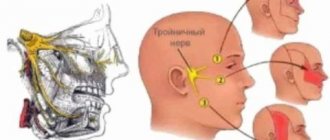
On the lower surface of the brain, the vagus nerve appears as 10-15 roots from the thickness of the medulla oblongata behind the olive. Directing laterally and downward, it leaves the skull through the anterior part of the jugular foramen along with the glossopharyngeal and accessory nerves, located between them. In the area of the jugular foramen, the vagus nerve thickens due to the upper node (lat. ganglion superius), and a little lower, after 1.0-1.5 cm, there is another node of somewhat larger size - lat. ganglion inferius.
In the interval between these nodes, the internal branch of the accessory nerve approaches it. Descending lower, the vagus nerve in the neck lies on the anterior posterior surface of the internal jugular vein (lat. v.jugularis interna) and follows to the upper aperture of the chest, located in the gutter between this vein and the internal carotid artery located more medially at first (lat. a. carotis interna), and then the common carotid artery (lat. a. carotis communis).
The vagus nerve with the internal jugular vein and the common carotid artery is enclosed in one common connective tissue sheath, forming the neurovascular bundle of the neck.
In the area of the upper thoracic outlet, the vagus nerve is located between the subclavian artery (lat. a.subclavia) (behind) and the subclavian vein (lat. v.subclavia) (in front).
Having entered the chest cavity, the left vagus nerve lies on the anterior surface of the aortic arch, and the right one lies on the anterior surface of the initial section of the right subclavian artery. Then both vagus nerves deviate somewhat backward, go around the posterior surface of the bronchi and approach the esophagus, where they scatter into a number of large and small nerve branches and lose the character of isolated nerve trunks.
The branches of the left and right vagus nerves are directed to the anterior (mainly from the left) and posterior (mainly from the right) surfaces of the esophagus and form the esophageal plexus (lat. plexus oesophageus).
From the branches of this plexus at the esophageal opening (Latin ostium oesophageum) of the diaphragm, the anterior and posterior vagal trunks (Latin trunci vagales anterior et posterior) are formed, respectively, which, together with the esophagus, penetrate into the abdominal cavity. Both the anterior and posterior trunk contain fibers of the left and right vagus nerves.
In the abdominal cavity, the vagal trunks send a series of branches to the abdominal organs and solar plexus.
According to its course, each vagus nerve is divided into four sections: head, cervical, thoracic and abdominal.
Head section of the vagus nerve
The cephalic section of the vagus nerve is the shortest, reaching the lower ganglion (lat. ganglion inferius). The following branches depart from it:
- The meningeal branch (lat. Ramus meningeus) departs directly from the superior node, goes into the cranial cavity and innervates the dura mater of the brain (transverse and occipital venous sinuses).
- The auricular branch (lat. Ramus auricularis), as a rule, starts from the upper node or lower - from the trunk of the nerve, goes posteriorly, follows the outer surface of the bulb of the internal jugular vein, approaches the jugular fossa (lat. fossa jugularis) and enters the mastoid canaliculus (lat. canaliculus mastoideus). In the thickness of the pyramid of the temporal bone, the auricular branch exchanges fibers with the facial nerve and leaves the pyramid of the temporal bone through the tympanomastoid fissure (lat. fissura tympanomastoidea). The auricular branch then divides into two branches that appear behind the outer ear, near the outer end of the bony portion of the external auditory canal. One of the branches connects to the posterior auricular nerve (lat. n.auricularis posterior) from the facial nerve, the other innervates the skin of the posterior wall of the external auditory canal.
- The connecting branch with the glossopharyngeal nerve (lat. Ramus communicans cum nervo glossopharyngeus), connects the upper node of the vagus nerve with the lower node of the glossopharyngeal nerve.
- The connecting branch with the accessory nerve (lat. Ramus communicans cum nervo accessorius) is represented by the internal branch of the accessory nerve. This is a rather powerful trunk that joins the vagus nerve between the upper and lower nodes. In addition, small branches from the vagus nerve are directed to the accessory nerve.
Cervical vagus nerve
| Cranial nerves |
| CHN 0 – Zero |
| CN I – Olfactory |
| CHN II – Visual |
| CN III – Oculomotor |
| CHN IV – Block |
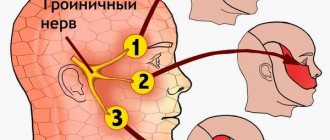
| CN V – Trigeminal |
| CN VI – Abductor |
| CHN VII – Facial |
| CN VIII – vestibulocochlear |
| CN IX – Glossopharyngeal |
| CHN X – Wandering |
| CHN XI – Additional |
| CN XII – Sublingual |
| Template: view • discussion • edit |
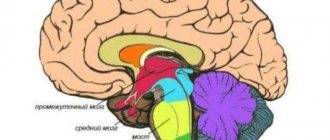
Diagram of the brain, brain stem and cranial nerves (vagus nerve marked in dark brown)
The cervical vagus nerve extends from the inferior ganglion to the origin of the recurrent laryngeal nerve (nervus laryngeus reccurens). Along this length, the following branches depart from the vagus nerve:
1. Pharyngeal branches (lat. Rr.pharyngei) often extend from the lower node, but can extend lower. There are two branches: the upper - large and the lower - smaller. The branches run along the outer surface of the internal carotid artery forward and somewhat inward, connecting with the branches of the glossopharyngeal nerve and the branches of the sympathetic trunk (Latin truncus sympathicus), forming a pharyngeal plexus (Latin plexus pharyngeus) on the middle constrictor of the pharynx. The branches extending from this plexus innervate the muscles and mucous membrane of the pharynx. In addition, nerves go from the superior branch to the muscle that lifts the velum palatine and to the muscle of the uvula.
2. The superior laryngeal nerve (lat. N.laryngeus superior) starts from the lower ganglion, goes down along the internal carotid artery, receiving branches from the superior cervical sympathetic ganglion (lat. ganglion cervicale superius) and the pharyngeal plexus, and approaches the lateral surface of the larynx. Before this, it splits into branches:
- external branch (lat. r.externus) innervates the mucous membrane of the pharynx, partly the thyroid gland, as well as the inferior pharyngeal constrictor and cricothyroid muscle, often this branch connects with the external carotid plexus
- the internal branch (lat. r.internus) goes along with the superior laryngeal artery, pierces the thyrohyoid membrane and with its branches innervates the mucous membrane of the larynx (above the glottis), epiglottis and partly the root of the tongue
- the connecting branch with the lower laryngeal nerve (lat. r.communicans (cum nervo laryngeo inferiori)) departs from the internal branch of the superior laryngeal nerve
3. The upper cervical cardiac nerves (lat. Nn.cardiaci cervicales superiores) in the amount of 2-3, depart from the trunk of the vagus nerve and are directed along the common carotid artery, and the branches of the right vagus nerve go in front of the brachiocephalic trunk (lat. truncus brachiocephalicus), left - in front of the aortic arch. Here they connect with the cardiac branches from the sympathetic trunk and, approaching the heart, form part of the cardiac plexus (lat. plexus cardiacus).
4. The lower cervical cardiac nerves (lat. Nn.cardiaci cervicales inferiores) are more numerous and much thicker than the upper ones, extending slightly below the recurrent laryngeal nerve. Heading towards the heart, the branches connect with the rest of the cardiac branches from the vagus nerve and from the sympathetic trunk and also take part in the formation of the cardiac plexus.
5. The recurrent laryngeal nerve (lat. N.laryngeus reccurens) departs from the main trunk on the right - at the level of the subclavian artery, and on the left - at the level of the aortic arch. Having circled the indicated vessels from below from front to back, they are directed upward in the groove between the trachea and esophagus, reaching the larynx with their terminal branches.
Along its length, the recurrent laryngeal nerve gives off a number of branches:
- tracheal branches (lat. rr.tracheales) are directed to the anterior surface of the lower part of the trachea. Along their course they connect with the sympathetic branches and approach the trachea;
- esophageal branches (lat. rr.esophagei) innervate the esophagus
- The lower laryngeal nerve (lat. n.laryngeus inferior) is the terminal branch of the recurrent laryngeal nerve. Along its course, it is divided into anterior and posterior branches. The anterior branch innervates the lateral cricoarytenoid, thyroarytenoid, thyroepiglottic, vocal and aryepiglottic muscles. The posterior or connecting branch with the internal laryngeal branch (lat. r.communicans cum nervo laryngeo superiori) contains both motor and sensory fibers. The latter approach the mucous membrane of the larynx below the glottis. Motor fibers of the posterior branch innervate the posterior cricoarytenoid and transverse arytenoid muscles
In addition, in the cervical region of the vagus nerve there are several more connecting branches:
- with superior cervical sympathetic ganglion
- with hypoglossal nerve
- between the recurrent laryngeal nerve and the cervicothoracic ganglion of the sympathetic trunk
Thoracic vagus nerve
The thoracic division of the vagus nerve begins at the origin of the recurrent laryngeal nerve and ends at its passage through the esophageal opening of the diaphragm. In the chest cavity it gives off the following branches:
- The thoracic cardiac branches (lat. Rr.cardiaci thoracici) begin below the recurrent laryngeal nerve, follow down and medially, connect with the lower cervical cardiac branches, send branches to the hilum of the lungs and enter the cardiac plexus.
- Bronchial branches (lat. Rr.bronchiales) are divided into less powerful anterior branches (4-5) and more powerful and numerous posterior branches
- The pulmonary plexus (lat. Plexus pulmonalis) is formed by the anterior and posterior bronchial branches connecting with the branches of the upper 3-4 thoracic sympathetic ganglia of the sympathetic trunk. The branches extending from the pulmonary plexus connect with each other and enter the gates of the lungs with bronchi and vessels, branching out in the parenchyma of the latter.
- The esophageal plexus (lat. Plexus esophageus) is represented by many nerves of varying diameters that extend from each vagus nerve below the root of the lung. Along their course, these branches connect with each other and with branches from the upper 4-5 thoracic nodes of the sympathetic trunks and form the esophageal plexus around the esophagus. It surrounds the entire lower part of the esophagus and sends some branches to its muscular and mucous membranes.
Abdominal vagus nerve
The abdominal part of the vagus nerve is represented by the anterior and posterior vagus trunks. Both trunks are formed from the esophageal plexus and along the anterior and posterior surfaces of the esophagus enter the abdominal cavity either in single trunks or in several branches.
The posterior trunk of the vagus nerve in the region of the cardia sends a number of branches - the posterior gastric branches (lat. rr.gastrici posteriores), to the posterior surface of the stomach, and itself deviates posteriorly, forming the celiac branches (lat. rr.celiaci), running along the left gastric artery to the solar plexus. The fibers that make up the celiac branches pass through the solar plexus to the abdominal organs.
The anterior trunk of the vagus nerve in the stomach area connects with the sympathetic nerves accompanying the left gastric artery and sends 1-3 branches between the leaves of the lesser omentum to the liver - hepatic branches (lat. rr.hepatici). The rest of the anterior trunk follows along the anterior periphery of the lesser curvature of the stomach and here gives off numerous anterior gastric branches (lat. rr.gastrici anteriores), to the anterior surface of the stomach.
Gastric branches from the anterior and posterior trunks in the subserosal layer form the anterior and posterior plexuses of the stomach.
Prevention
To prevent diseases of the vagus nerve, there is no need to adhere to some complex diet or douse yourself with cold water. All recommendations are quite adequate and will not cause difficulties for the average person. So, the recommendations include:
- Maintaining a healthy lifestyle.
- Daily moderate physical activity.
- Daily healthy sleep.
- Take a contrast shower in the evening.
- Rejection of bad habits.
- Avoiding stressful situations at work.
So why is it so important to take care of your emotional well-being? Because a calm and balanced person is much less likely to suffer from illnesses, including illnesses associated with inflammation of the vagus nerve. Take care of your nerves, it will be much harder to treat them than to save them.
Source: https://nervivporyadke.ru/
Function
The vagus nerve is mixed, as it contains motor, sensory and parasympathetic fibers. Accordingly, fibers from several cores pass through it. It should be noted that from the nuclei in which the fibers of the vagus nerve begin, the fibers of the glossopharyngeal and accessory nerves also originate.
Motor fibers originate from the double nucleus (lat. nucleus ambiguus), common with the glossopharyngeal and accessory nerves. It is located in the reticular formation, deeper than the posterior nucleus of the vagus nerve in the projection of the triangle of the vagus nerve (lat. trigonum n.vagi). It receives supranuclear impulses from both hemispheres of the brain along the corticonuclear pathways. Therefore, unilateral interruption of the central fibers does not lead to a significant disruption of its function. The axons of the nucleus innervate the muscles of the soft palate, pharynx, larynx, as well as the striated muscles of the upper part of the esophagus. The double nucleus receives impulses from the spinal nucleus of the trigeminal nerve (lat. nucleus tractus spinalis n.trigemini) and from the nucleus of the solitary tract (lat. nucleus tractus solitarii) (relay point for taste fibers). These nuclei are parts of reflex arcs starting from the mucous membrane of the respiratory and digestive tracts and are responsible for the occurrence of cough and vomiting.
The dorsal nucleus of the vagus nerve (lat. Nucleus dorsalis n.vagi) is located deep in the triangle of the vagus nerve of the rhomboid fossa. The axons of the posterior nucleus of the vagus nerve are preganglionic parasympathetic fibers. Short postganglionic fibers send motor impulses to the smooth muscles of the lungs, intestines, down to the splenic flexure of the colon, and to the heart muscle. Stimulation of these parasympathetic fibers causes a slowdown in heart rate and contraction of bronchial smooth muscles. In the digestive tract, there is an increase in the secretion of the glands of the mucous membrane of the stomach and pancreas.
The posterior nucleus of the vagus nerve receives afferent impulses from the hypothalamus, the olfactory system, the autonomic centers of the reticular formation and the nucleus of the solitary tract. Impulses from baroreceptors in the wall of the carotid glomus are transmitted along the glossopharyngeal nerve and are involved in the regulation of blood pressure. Chemoreceptors in the carotid tangle take part in the regulation of oxygen tension in the blood. The receptors of the aortic arch and para-aortic bodies have similar functions; they transmit their impulses along the vagus nerve.
It should be noted that postganglionic sympathetic fibers from the cells of the paravertebral sympathetic ganglia also enter the vagus nerve and spread along its branches to the heart, blood vessels and internal organs.
The nucleus alae cinereae contains the bodies of the second neurons of general sensitivity, common to the glossopharyngeal and vagus nerves. The bodies of the first neurons are located in the superior and inferior ganglia of these nerves, which are located in the region of the jugular foramen. Afferent (sensitive) fibers of the vagus nerve innervate the mucous membrane of the lower part of the pharynx and larynx, the area of skin behind the ear and part of the external auditory canal, the eardrum and the dura mater of the posterior cranial fossa.
Stimulation
The vagus plays an important role in the human body. So, in his normal state he:
- improves blood sugar regulation;
- reduces the risk of stroke and heart disease;
- stabilizes blood pressure;
- improves digestion;
- reduces the intensity and number of attacks of headaches and migraines;
- lifts the mood;
- reduces stress and anxiety.
In order to maintain good tone of the vagus nerve, it is recommended to regularly activate it (this procedure is called vagus nerve stimulation).
Stimulation promotes:
- reducing the risk of panic attacks, fears, and heart disease;
- prevention of Alzheimer's disease;
- combating headaches, excess weight and obesity;
- encouraging the body to fight bulimia, anorexia, autoimmune diseases, cancer, hemorrhoids;
- eliminating problems with alcoholism.
You must understand that ordinary activation of the vagus is not enough to overcome this or that disease, but in combination with drug treatment it shows good results.
Stimulation option
Activation is possible in the following ways:
- slow and rhythmic belly breathing (10–15 minutes);
- meditation (15–20 minutes);
- washing with cold water (morning and evening);
- taking probiotics;
- gargling (repeated several times a day after meals);
- singing (loudly and with pleasure, and this also has a positive effect on the parasympathetic system);
- taking fish oil (Omega 3 is an excellent stimulant).
Clinic of vagus nerve lesions
The causes of damage to the vagus nerve can be both intracranial and peripheral. Intracranial causes include tumor, hematoma, thrombosis, multiple sclerosis, syphilis, amyotrophic lateral sclerosis, syringobulbia, meningitis, and aneurysm. Peripheral causes may be neuritis (alcoholic, diphtheria, lead, arsenic poisoning), tumor, glandular diseases, trauma, aortic aneurysm.
Bilateral complete vagus nerve palsy is rapidly fatal. With a unilateral lesion, there is a drooping of the soft palate on the affected side, immobility or lag on this half when pronouncing the sound “a”. The tongue is deviated to the healthy side. In addition, with unilateral damage to the vagus nerve, paralysis of the vocal cord is observed - the voice becomes hoarse. The pharyngeal reflex from the mucous membrane of the affected side of the pharynx may be lost. In addition, slight dysphagia and temporary tachycardia and arrhythmia may be observed.
A bilateral decrease in the function of the vagus nerves can cause a speech disorder in the form of aphonia (the voice loses sonority as a result of paralysis or severe paresis of the vocal cords) or dysarthria (due to paresis of the muscles of the speech motor apparatus, a decrease in sonority and a change in the timbre of the voice, impaired articulation of vowels and especially consonants, nasal tone of speech). Dysphagia is also characteristic - a swallowing disorder (choking on liquid food, difficulty swallowing any food, especially liquid). This whole triad of symptoms (dysphonia, dysarthria, dysphagia) is due to the fact that the vagus nerve carries motor fibers to the striated muscles of the pharynx, soft palate and velum, epiglottis, which are responsible for the act of swallowing and human speech. A weakening of the swallowing reflex leads to the accumulation of saliva and sometimes food in the patient’s mouth, and a decrease in the cough reflex when liquid and pieces of solid food enter the larynx. All this creates conditions for the development of aspiration pneumonia in the patient.
Since the vagus nerves carry parasympathetic fibers to all organs of the thoracic cavity and most abdominal organs, their irritation can lead to bradycardia, broncho- and esophageal spasms, increased peristalsis, increased secretion of gastric and duodenal juice, etc. Decreased function of these nerves leads to breathing disorders, tachycardia, inhibition of the enzymatic activity of the glandular apparatus of the digestive tract, etc.
Diagnostics
Diagnosis of the disease is carried out in a medical institution and begins with interviewing the patient and clarifying what is bothering him. For example, in case of problems with swallowing, the doctor examines the soft palate (the tongue sags in the direction opposite to the lesion) and the throat. In addition, the doctor evaluates the timbre of the voice and the level of wheezing during pronunciation.
To check the swallowing function, it is enough to ask the patient to drink a glass of water; during swallowing, a cough should begin (a natural reaction of the body in case of neuritis of the vagus nerve with complications of swallowing function).
In addition, the neurologist additionally prescribes:
- laryngoscopy;
- magnetic resonance imaging (MRI);
- radiography;
- ECG.
Research methodology
Determine the sonority of the voice, which may be weakened or completely absent (aphonia); At the same time, the purity of pronunciation of sounds is checked. The patient is asked to pronounce the sound “a”, say a few words, and then open his mouth. They examine the palate and uvula, determine whether there is a drooping soft palate, and whether the uvula is symmetrically located.
To determine the nature of the contraction of the soft palate, the subject is asked to pronounce the sound “e” with his mouth wide open. In case of damage to the n.vagus, the palatine velum lags behind on the side of paralysis. The palatal and pharyngeal reflexes are examined using a spatula. It should be borne in mind that a bilateral decrease in the pharyngeal reflex and the soft palate reflex can also occur normally. Their decrease or absence on one side is an indicator of damage to pairs IX and X.
Swallowing function is tested by taking a sip of water or tea. If dysphagia is present, the patient will choke on just one sip of water.
To determine the condition of the vocal cords, laryngoscopy is performed.
Treatment
It is necessary to act immediately in the case of disorders associated with the vagus, since the lack of treatment can lead to dire consequences.
Treatment is divided into conservative and surgical. In addition, folk remedies can be placed in a separate category.
Conservative treatment involves taking hormonal drugs (prednisolone, hydrocortisone) that help eliminate symptoms.
In addition, in order to calm the pain, we can take painkillers.
It is permissible to treat inflammation of the vagus nerve with antihistamines, which relieve swelling that has formed around the vagal nerve.
Naturally, vitamin supplementation is necessary for the affected nerve and weakened body. A suitable vitamin for this is vitamin B, as well as preparations containing magnesium.
As in most cases, after a course of drug therapy, physiotherapeutic procedures are necessary, which include:
- Diadynamic currents (have a stimulating effect on muscles).
- Plasmaphoresis.
- Electrical stimulation.
As a rule, the effect of physiotherapy at the treatment stage is minimal, so this type of therapy is used as a restorative procedure.
Additionally, you can resort to traditional medicine recipes. It is difficult to cure a disease using only home treatment methods, and it is not recommended to replace drug therapy with traditional ones. Taken together, there can be some pretty good results.
The main home treatment options include:
- Baths.
- Tinctures.
- Decoctions.
- Mono-products.
Herbal baths - mix 20 g of calamus, oregano, pine buds and yarrow in equal proportions and pour the resulting mixture into 5 liters of hot water. Before pouring the resulting mixture into the bath, leave it for up to 5 hours. You should take a bath for no more than 20 minutes. It is believed that such manipulations relax muscle tone and help calm the nerve.
There are many types of baths; as an alternative, you can try using valerian root and sage, also mixed in equal proportions and infused with boiling water.
Sedative decoctions are used as a means of oral administration. So, to prepare a sedative, you need to mix 10 g of mint and lemon balm in equal proportions and pour 300 ml of hot boiled water over them. This decoction should steep for at least an hour. Use the product every day, one glass.
To relieve nervous tension, just boil a tbsp in 50 ml of water. a spoonful of thyme flowers. It is better to take this decoction every day, 50 ml.
The patient can make a pillow for himself from soothing herbs. This product is called an aromatic pillow. Herbs that can be used include:
- thyme;
- mint;
- Melissa;
- hop cones;
- chamomile;
- Bay leaf;
- oregano;
- lavender.
Single-use medications include honey, which must be taken regularly instead of sugar. Honey has a restorative and calming effect when taken regularly. Homeopathy also shows good results.
Surgical intervention is resorted to as a last resort, when conservative treatment does not bring visible results. In addition, surgical intervention is indicated for people with tumor processes; tumor removal is in some cases a prerequisite for recovery. The surgeon must make sure that the operation will do more good than harm.