Causes
- Crutch paralysis (pressure in the armpit)
- “Saturday Night Palsy” (falling asleep with your hand on the back of a chair, compressing the radial nerve in the armpit)
- Traumatic injury
- Iatrogenic trauma (eg, plate fixation of the proximal radius or ulna)
- Traction injury (eg, Holstein-Lewis fracture = oblique fracture of the distal third of the humerus).
Symptoms and signs
Mild weakness of elbow flexion - brachioradialis muscle. Noticeable weakness of elbow extension, wrist extension, finger extension at the metacarpophalangeal joint, retroposition of the first finger. Numbness along the back of the first ray at the base. The ability to extend the nail phalanx of the first finger is preserved (the abductor pollicis brevis muscle and the adductor muscle through the tendon stretch of the extensor apparatus).
Treatment
- Pressure paralysis: an observation. Recovery occurs after a few hours, but sometimes after weeks or months. If there is no recovery, tendon transposition is indicated.
- Intersection: emergency restoration or plastic surgery.
- For a shoulder fracture:
- Observation: For closed low-energy trauma, surgery is not indicated. If there is no recovery, an EMG is performed after 6-12 weeks. In case of denervation, surgical intervention is necessary.
Operation: open injury; high energy trauma; in case of secondary damage (paresis of a primarily intact nerve after repositioning of the shoulder).
If nerve repair is unsuccessful, tendon transposition is indicated.
Compression of the posterior interosseous nerve
Causes
Brachial plexus neuritis (Parsonage-Turner syndrome): without compression neuropathy in the forearm, but with dysfunction of part of the brachial plexus, often preceded by a viral infection and shoulder/neck pain.
Spontaneous compression in the radial canal:
- Fibrous proximal border of the extensor carpi radialis brevis
- Arcade of Frohse (proximal edge of the instep support)
- Distal edge of the instep support
- Recurrent radial branch of vessels
External compression:
- Lipoma
- Synovitis of the proximal radioulnar joint or capitate-radial joint
Symptoms and signs
Weakness of the hand and wrist often develops quickly. Shoulder pain or viral infection (brachial plexus neuritis).
Extension at the wrist is preserved, but movements are directed to the radial side; there is no extension in the metacarpophalangeal joints of the three-phalangeal fingers. There is no retroposition of the first toe.
Compensatory movements:
- Extension in the proximal interphalangeal joints is preserved due to the function of the short muscles of the hand - the ulnar nerve
- The ability to extend the nail phalanx of the first finger (flexor pollicis brevis, abductor brevis, opponens pollicis brevis and adductor muscles through the tendon extension of the extensor apparatus) is preserved.
- Extending the fingers using their own weight to enhance the effect of passive tenodesis in wrist flexion.
- Wrist extension occurs by relaxing the wrist flexors against gravity.
Survey
- MRI or ultrasound of the anterior cubital fossa to exclude causes of nerve compression
- Nerve function testing - insertional electromyography.
Conservative treatment
Observation: In the absence of a tumor and possible brachial plexus neuritis, observation is indicated. May require 12 months.
Splinting:
- Splint that holds the wrist in extension
- Dynamic splinting in extension
- Tenodesis splinting (based on the tenodesis effect)
Operation
Dorsal radial access. Cosmetically preferable. Find the space between the extensor digitorum communis and the extensor carpi ulnaris distally and continue the selection proximally. Cross the superficial part of the instep, release the edge of the short extensor carpi radialis, and ligate the vessels crossing the nerve.
Anterior approach: S-shaped incision through the anterior cubital fossa. Identify the posterior interosseous nerve between the brachialis and brachioradialis muscles and retract distally; cut the edge of the short extensor carpi radialis and the superficial plate of the supinator, ligate the vessels crossing the nerve. A large scar remains, prone to hypertrophy.
Tendon transposition: If there is no recovery of the nerve, a tendon transposition is performed, which is used for radial nerve injury.
Radial tunnel syndrome
Causes
There are conflicting opinions about the existence of this syndrome. The pathology is unclear. The posterior interosseous nerve, although it provides only motor function, contains a large percentage of sensory nerve fibers.
Symptoms
- Pain in the extensor muscle region (upper outer part of the forearm) behind the lateral epicondyle.
- It worsens with exercise and goes away after rest.
- No specific extensor weakness is noted.
- May be mistaken for tennis elbow.
Signs
- There are no motor disorders.
- Pain on palpation of the extensor muscles.
- Sometimes pain occurs when extending the wrist or supinating or extending the third finger with resistance.
Survey
- Nerve examination: normal, not indicated
- Local anesthesia under the muscular part of the extensor muscles - a temporary decrease in symptoms confirms the diagnosis
Treatment
- Observation: Spontaneous resolution is possible and no other treatment is available.
- Treat associated tennis elbow (cortisone injection, elastic elbow pad, ultrasound)
- Surgery: performed for persistent symptoms consistent with this syndrome. Dorsal radial access (described above); improvement is not guaranteed.
Prevention
To avoid the development of neuralgia of the radial nerve of the left or right hand, and especially necrosis, we must not forget about disease prevention. Since it develops not only after injuries, but also due to metabolic disorders. It is also observed with insufficient physical activity.
As a preventative measure, various hand injuries and hypothermia should be avoided. It is also recommended to promptly treat all infectious diseases and vaccinate. In order to maintain immunity, you need to eat right, exercise, follow a work and rest schedule, and lead a healthy lifestyle.
Neuritis of the hand manifests itself with pronounced symptoms, but can be treated without difficulty. The main goal of therapy is to restore impaired blood circulation. If you consult a specialist in a timely manner, the disease goes away without a trace and there are no consequences. But you should remember that self-medication is strictly prohibited.
Wartenburg syndrome
Very rare.
Causes
- Compression of the superficial radial nerve where it exits from under the brachioradialis muscle into the subcutaneous tissue along the radial edge of the distal forearm.
- Causes: spontaneous appearance; watch or bracelet pressure; handcuffs; direct blow.
- Differential diagnosis: de Quervain's disease, crossover syndrome (crepitating tenosynovitis), arthritis of the saddle joint
Symptoms and signs
- Tingling along the rear of the first ray
- Tinel's percussion test is positive over the nerve (more than on the healthy side - this nerve is always very sensitive)
- Decreased conductivity on electrophysiological examination
Treatment
- Avoid pressure from watches and bracelets
- Surgical decompression. Dorsal radial access. The superficial radial nerve is identified and released at the point where it emerges from the brachioradialis tendon.
Radial nerve disease (neuropathy) (G56.3) is a pathological condition in which the radial nerve is affected. It manifests itself as difficulty in straightening the muscles of the forearm, wrist, fingers, difficulty in abducting the thumb, and impaired sensitivity in the area of innervation of this nerve.
Etiology of radial nerve neuropathy: compression of the radial nerve during sleep (deep sleep, severe fatigue, alcohol intoxication); humerus fracture; long periods of walking with the help of crutches; past infections; intoxication.
Forecast and recovery
The recovery time for the radial nerve of the arm takes on average 1 – 2 months. The duration of rehabilitation is determined by the patient’s age, the nature of the lesion and the characteristics of concomitant diseases. Post-traumatic neuropathy requires a longer recovery.
To prevent neuropathy, you need to sleep in a comfortable position and give up bad habits. Persons whose profession involves frequent repetitive movements should regularly exercise and massage the upper extremities. It is also recommended to undergo a complete body examination every 6 months.
Radial nerve neuropathy (neuropathy) is a pathological condition of the upper extremities in which one of the three main nerves is damaged. This is the most common disease associated with hand damage.
From a functional point of view, the radial nerve influences the motor activity of the upper extremities: it promotes flexion and extension movements of the arm and phalanges of the fingers, and is responsible for the ability to move the thumbs to the side.
The fibers of the radial nerve interact with the cutaneous nerve formations of the forearm and shoulder.
Radiation neuropathy is most often a secondary phenomenon and occurs due to muscle overload and traumatic injury. Most often, traumatologists, orthopedists, specialists in the field of sports medicine and neurology encounter this pathology.
Causes
The main cause of damage to the radial nerve is compression. This is due to various circumstances:
- A special position of the hand when it lies under the head or is pressed down by the body for a long period of time. Typically, this condition can be caused by extreme fatigue or heavy sleep, often under the influence of alcohol intoxication.
- The appearance of scars in the muscles along the radial nerve due to strong impacts.
- Prolonged impact on the arm when using crutches.
- Shoulder bone fractures.
- By tightening the arm with a tourniquet for a long time.
- Incorrect position of the nerve.
- Injection intervention in the shoulder area.
In some cases, radiation neuropathy is a consequence of:
- Alcohol poisoning of the body during prolonged drinking bouts.
- Hormonal imbalances in women and pregnancy.
- Intoxication of the body by exposure to lead.
- Past infectious diseases.
- Development of diabetes mellitus.
Dysfunction of the radial nerve of the upper extremities may be associated with the professional characteristics of a person’s life. Thus, among patients with this disease, a large percentage are those whose activities involve manual labor, including physical labor.
Professional athletes often suffer from neuropathy; for example, while running, a person has to sharply bend his elbows many times. Or is it due to the constant arm movements of professional tennis players. Prolonged stress can cause disruption in the functioning of nerve structures.
Symptoms
The symptoms of the disease largely depend on the location of the damage. There are several types of neuropathy, each of which is characterized by a specific set of symptoms.
First type
The armpit area is damaged. This is the so-called crutch paralysis. Immobilization of the forearm muscles occurs, the process of flexion and extension of the limb is disrupted, and the triceps muscle, which plays an important role in straightening the forearm, atrophies.
If this particular part of a person’s hand is injured, the following occurs:
- The hand droops when raising the arm.
- When the arm is extended, there is difficulty in straightening the wrist.
- The first and second fingers are closed.
- Fingers lose sensitivity and a state of numbness occurs.
Second type
This is the most common type of radiation neuropathy, which occurs when a nerve is accidentally damaged: during sound sleep, due to prolonged exposure of the arm in a certain position during anesthesia, application of a tourniquet, or a fracture of the shoulder. Even prolonged exposure to an uncomfortable position can cause this type of nerve damage.
When the nerve in the middle part of the shoulder is compressed, symptoms such as a feeling of numbness on the back of the hand and the inability to straighten the fingers appear. But extension movements in the forearm area are preserved.
Third type
With this type of disease, damage to the posterior process of the nerve occurs, which manifests itself in damage to the limb in the elbow area. A chronic course is often observed due to weakening of the joint ligaments and changes in the functionality of the hand muscles. When extending the elbow, pain is felt in the muscles of the forearm. Pain occurs when moving the hand.
General symptoms
With each type of neuropathy, main and accompanying symptoms appear. The main ones are those that were discussed earlier.
Associated symptoms are common to all types of nerve damage. These include:
- swelling at the site of the lesion;
- the occurrence of difficulties when performing motor actions with the hands;
- impaired coordination of hand movements;
- decreased sensitivity;
- spasms and convulsions.
If such signs occur, it is necessary to urgently take action and begin treatment.
Diagnostics
In order to prescribe the correct treatment, it is necessary to find out where the limb injury occurred. In addition, at this stage it is important to identify which nerve is damaged.
When the doctor, using functional tests and sensitivity studies, accurately determines that he is dealing with the radial nerve, a set of measures is prescribed to determine the location of the lesion. In this case, electromyography and electroneurography are used to diagnose a decrease in the functional activity of muscle contractions and a slowdown in the passage of nerve impulses along the nerve.
When making a diagnosis, the attending physician takes into account the nature and causes of the disease, among which toxic, ischemic, post-traumatic, and compression lesions can be highlighted.
It is important to conduct additional consultations with specialists: orthopedist, endocrinologist, traumatologist. The doctor gives a referral to take tests for the biochemical composition of the blood, and also examines the level of sugar in the blood.
Treatment
Treatment options for radiation neuropathy depend on which part of the arm the lesion occurs in and what caused the impairment. If neuropathy is a consequence of intoxication of the body or the result of infectious diseases a person has suffered, drug treatment is necessary.
In the case of traumatic events, for example, fractures, it is important to ensure complete immobilization of the limb and carry out the necessary procedures related to the elimination of the injury.
Typically, a fracture results in a severed nerve. It becomes inevitable to carry out an operation—surgical actions to stitch the nerve. In this case, it is necessary to detect the hand injury as soon as possible. The earlier the diagnosis is made, the faster the damaged nerve will be restored.
If nerve neuropathy is caused by external influences and appears, for example, as a result of active muscle activity, the use of crutches or sleeping in an unusual position, then negative factors should be abandoned during rehabilitation treatment.
Typically, patients with this diagnosis are observed on an outpatient basis, and hospitalization is required only for patients who require the use of potent painkillers.
Drug therapy involves taking medications such as:
- anti-inflammatory drugs that eliminate pain and relieve inflammation;
- decongestants - to relieve swelling;
- vasodilators, which cause blood flow and improve nutrition of muscles and nerves;
- biostimulant drugs and B vitamins that promote the restoration and healing of damaged nerve areas.
Traditional drug therapy for neuropathy must necessarily be accompanied by additional physiotherapeutic procedures: therapeutic exercises, massage, acupuncture, magnetotherapy, electromyostimulation, electrophoresis using medicinal solutions.
Massage and physical therapy play an important role in restorative procedures for the radial nerve and the return of lost hand functions. A whole range of different exercises has been developed aimed at restoring motor activity of the hand. Exercises are selected individually, depending on the nature of the damage, and the load increases gradually.
The effectiveness of using devices made of rubber or with a spring mechanism, which develop joints, causing them to move, has been proven. One of the most effective ways to restore a damaged arm is a set of gymnastic exercises in water.
Physiotherapy
Along with traditional drug treatment, a certain set of exercises is often prescribed, which can significantly speed up the rehabilitation process.
The exercises are easy to perform, do not require much time and can be performed anywhere. The main thing is a systematic approach and perseverance in achieving the goal. The therapeutic effect of restorative physical education will become noticeable after the first days of classes.
You need to do the following exercises every day:
- Bend your arm at the elbow joint and place it on the surface of a table or any other surface (while placing your forearm at a right angle to the table). Slowly lower your thumb and try to raise your index finger. Perform these movements one by one 10 times.
- The hand position is similar to the first exercise. The index finger goes down and the middle finger goes up. Perform the movements alternately 10 times.
- Take the phalanges of the four fingers of the injured hand with the fingers of your healthy hand (try to keep the thumb on the palm side). Bend and extend the main phalanges of the captured fingers with your healthy hand. After this, with your healthy hand, clench the fingers of the affected hand into a fist, and then straighten them. All manipulations with the fingers must be done 10 times.
There is a whole range of restorative exercises in water that have an excellent healing effect. Water has special healing properties: when a person performs movements with a sore arm, water creates a certain resistance, overcoming which one has to make an effort and thereby develop the injured limb.
Clinical picture
Patients are concerned about pain and a tingling sensation, burning sensation in the fingers and back of the forearm, weakness in the muscles of the hand. Gradually, numbness of the back of the hand appears, adduction and abduction of the thumb is impaired, and extension of the hand and forearm becomes difficult.
An objective examination of the patient reveals:
- paresthesia and hypoesthesia in the area of the rear of the I, II, III fingers, the posterior surface of the forearm (70%);
- weakness in the extensor muscles of the hand and fingers, weakness of the supinator, brachioradialis muscle (60%);
- inability to abduct and adduct the thumb (70%);
- decreased carporadial reflex (50%);
- muscle atrophy (40%);
- the appearance of pain during supination of the forearm with overcoming resistance and in the test with extension of the middle finger (50%);
- pain on palpation along the radial nerve (60%).
Treatment of radial nerve damage
- Nonsteroidal anti-inflammatory drugs, vitamins.
- Physiotherapy, massage.
- Temporary limitation of physical activity on the arm.
- Novocaine and hydrocortisone blockades.
- Surgical treatment (used for compression of the radial nerve).
Treatment is prescribed only after confirmation of the diagnosis by a medical specialist.
Essential drugs
There are contraindications. Specialist consultation is required.
- Xefocam (non-steroidal anti-inflammatory drug). Dosage regimen: for relief of acute pain syndrome, the recommended oral dose is 8-16 mg/day. in 2-3 doses. The maximum daily dose is 16 mg. The tablets are taken before meals with a glass of water.
- (analgesic). Dosage regimen: IV, IM, SC in a single dose of 50-100 mg, possible repeated administration of the drug after 4-6 hours. The maximum daily dose is 400 mg.
- (non-steroidal anti-inflammatory drug). Dosage regimen: IM - 100 mg 1-2 times a day; after pain relief, it is prescribed orally in a daily dose of 300 mg in 2-3 doses, a maintenance dose of 150-200 mg/day.
- (a diuretic from the group of carbonic anhydrase inhibitors). Dosage regimen: adults are prescribed 250-500 mg once in the morning for 3 days, on the 4th day - a break.
- (vitamin B complex). Dosage regimen: therapy begins with 2 ml intramuscularly 1 time per day for 5-10 days. Maintenance therapy - 2 ml IM two or three times a week.
- Prozerin (inhibitor of acetylcholinesterase and pseudocholinesterase). Dosage regimen: orally for adults, 10-15 mg 2-3 times a day; subcutaneously - 1-2 mg 1-2 times a day.
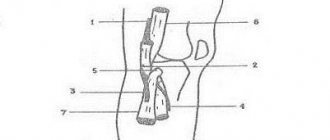
Table of contents of the topic “Brachial plexus, plexus brachialis”:
Radial nerve, n. radialis. Medial cutaneous nerve of the forearm, n. cutaneus antebrachii medialis.
Medial cutaneous nerve of the forearm, n. cutaneus antebrachii medialis
also from the medial bundle of the plexus (from C8, Th1), in the axillary fossa lies next to n. ulnaris; in the upper part of the shoulder is located medial to the brachial artery next to v. basilica, together with which it pierces the fascia and becomes subcutaneous. This nerve innervates the skin on the ulnar (medial) side of the forearm to the wrist joint.
N. radialis, radial nerve
(C5-C8, Th1), forms a continuation of the posterior bundle of the brachial plexus.
It passes behind the brachial artery along with a. profunda brachii on the back side of the shoulder, spirals around the humerus, located in the canalis humeromuscularis, and then, piercing the lateral intermuscular septum from back to front, exits into the space between m. brachioradialis and m. brachialis. Here the nerve divides into superficial ( ramus superficialis
) and deep (
ramus profundus
) branches.
Before this n.
radialis gives the following branches:
Rami musculares
on the shoulder for extensors - m. triceps and m. anconeus. The last branch also supplies the capsule of the elbow joint and the lateral epicondyle of the shoulder, so when the latter becomes inflamed (epicondylitis), pain occurs along the entire radial nerve.
Nn. cutanei brachii posterior et lateralis inferior
branch in the skin of the posterior and lower part of the posterolateral surfaces of the shoulder.
N. cutaneus anterbrachii posterior
originates from the radial nerve in the canalis humeromuscularis, exits under the skin above the beginning of m. brachioradialis and extends to the dorsum of the forearm.
Rami musculares
go to m. brachioradialis, etc. extensor carpi radialis longus.
Ramus superficialis
goes to the forearm in the sulcus radialis lateral to a.
radialis, and then in the lower third of the forearm through the gap between the radius and tendon m. brachioradialis passes to the back of the hand and supplies five dorsal branches, nn.
digitales dorsales , on the sides of fingers I and II, as well as the radial side of III.
These branches usually end at the level of the last interphalangeal joints. Thus, each finger is supplied by two dorsal and two palmar nerves running on both sides. Dorsal nerves originate from n. radialis
and
n.
ulnaris , innervating each 2 1/2 fingers, and the palmar ones - from
n.
medianus and
n.
ulnaris , with the first supplying 3 1/2 fingers (starting with the thumb), and the second supplying the remaining 1 1/2 fingers.
Ramus profundus
passes through m.
supinator and, having supplied the latter with a branch, goes to the dorsal side of the forearm, innervating m. extensor carpi radialis brevis and all posterior muscles of the forearm. Continuation of the deep branch, n.
interosseus (antebrachii) posterior , descends between the extensors of the thumb to the wrist joint, which innervates.
From move n. radialis
it is clear that it innervates all extensors on both the shoulder and forearm, and on the latter also the radial muscle group. Accordingly, the skin on the extensor side of the shoulder and forearm is also innervated by it. The radial nerve, a continuation of the posterior bundle, is like the posterior nerve of the arm.
12. Damage to the radial nerve
This pathology occurs more often than other lesions of the nerves of the upper limb. Nerve damage is caused by a number of reasons. The nerve can be affected during sleep if the patient sleeps on a hard surface with his arm under his head or under his torso.
Basically, such a lesion occurs during deep sleep, which may be associated with intoxication or fatigue. This is the so-called sleep paralysis. Also, neuropathy of the radial nerve can occur under the influence of prolonged compression by a crutch or tourniquet as a result of fractures of the humerus. In some cases, radial nerve neuropathy can occur due to improper injection technique into the outer shoulder, which can occur if the nerve is abnormally located.
In fairly rare cases, factors that provoke damage to the radial nerve may be diseases (such as influenza, pneumonia, typhus, etc.) or intoxication (for example, alcohol or lead poisoning). The radial nerve is mixed in its function. The motor fibers included in its composition innervate the muscles - extensors of the forearm, which include the triceps, ulnaris, hand muscles: radial extensors of the wrist (short and long), extensor digitorum, extensor of the little finger, abductor pollicis longus, supinator. Innervating the above muscles, the nerve carries out the following motor functions: extension at the elbow joint, at the wrist joint, extension of the main phalanges of the fingers, abduction of the thumb, supination of the hand.
Sensory fibers of the radial nerve are part of the following cutaneous nerves: posterior cutaneous nerve of the shoulder, inferior lateral cutaneous nerve of the shoulder, posterior cutaneous nerve of the forearm. Sensitive fibers of the radial nerve are involved in the innervation of the skin on the posterior surface of the shoulder and forearm, the radial side of the hand, and the dorsum of the 1st, 2nd and 3rd fingers.
When the radial nerve is damaged at different levels, various clinical manifestations will be observed. The radial nerve can be affected in the axilla, upper third, middle third and lower third of the shoulder. Damage to the nerve in the armpit and upper third of the shoulder leads to the development of paralysis of the muscles receiving innervation from its fibers.
The following clinical picture is characteristic: there is a drooping of the hand when raising the arm, the first finger of the hand is brought to the second. The patient cannot straighten the forearm and hand, as the function of the extensor muscles is impaired. There is an inability to abduct the first finger of the hand and supination of the forearm. During the examination, loss of the ulnar extensor reflex is noted, as well as a decrease in the carporadial reflex. All types of sensitivity on the skin of the first, second and half of the third finger of the hand are impaired. Sensitivity disorders are most often expressed in the form of paresthesia.
Damage to the radial nerve in the middle third of the shoulder is clinically characterized by preservation of forearm extension, as well as the ulnar extensor reflex. Sensitivity on the skin of the shoulder is preserved.
An objective examination reveals all other symptoms of damage to the ulnar nerve. Damage to the radial nerve in the region of the lower third of the shoulder and upper third of the forearm is clinically characterized by the preservation of all types of sensitivity on the skin of the posterior surface of the forearm. Sensitivity on the skin of the back of the hand is impaired or completely lost, as well as the function of the extensor muscles of the hand and fingers.
Several diagnostic tests are necessary to determine whether there is radial nerve damage. If the patient's arms are stretched or raised upward, there is a drooping of the hand on the affected side. With the arm lowered, the patient cannot abduct the first finger and cannot supinate the hand. If you ask the patient to press his palms together and try to spread his fingers, then on the affected side the fingers will bend and slide along the palm of the healthy hand. The patient cannot abduct the first finger of the hand and simultaneously touch any plane with the back of the hand.
From the book Nervous Diseases by M.V. Drozdov by A.A. Drozdov From the book Nervous Diseases: Lecture Notes by the author A.A. Drozdov From the book Nervous Diseases: Lecture Notes by the author A.A. Drozdov From the book Nervous Diseases: Lecture Notes by the author A. A. Drozdov author Galina Yuryevna LazarevaFrom the book Paramedic Handbook author Galina Yuryevna LazarevaFrom the book Paramedic Handbook author Galina Yuryevna Lazareva author Vladimir Ivanovich VasichkinFrom the book Great Guide to Massage author Vladimir Ivanovich VasichkinFrom the book Great Guide to Massage author Vladimir Ivanovich VasichkinFrom the book Great Guide to Massage author Vladimir Ivanovich Vasichkin author Vladimir Ivanovich Vasichkin From the book Massage. Lessons from the great master author Vladimir Ivanovich VasichkinFrom the book Massage. Lessons from the great master author Vladimir Ivanovich VasichkinFrom the book Massage. Lessons from the great master author Vladimir Ivanovich Vasichkin
The radial nerve includes motor fibers that innervate the extensor muscles of the forearm.
These muscles include:
- muscle of the hand (extensor of the little finger, supinator, extensor of the fingers, radial extensors of the wrist: long and short, long muscle that abducts the thumb),
- elbow muscle,
- triceps
How does the disease manifest?
Symptoms of radial nerve neuropathy can be different - depending on the location and degree of the pathological process, the disease is manifested by disturbances in sensitivity, motor and autonomic functions of the hand.
- Motor manifestations. Patients with this diagnosis have difficulty extending the hand and elbow, and the ability to move the forearm is slightly impaired.
- Sensitive manifestations. Severe pain syndrome occurs in the area of the muscles of the forearm and elbow, manifests itself with intense movement of the hand and fingers (especially when trying to bend and straighten them), and burning pain in the area of the thumb is also possible, which spreads to the entire arm up to the forearm and shoulder.
- Vegetative manifestations. One of the symptoms of the disease is numbness and a crawling sensation on the skin; the most common is loss of sensation on the back of the hand and mild numbness of the shoulder.
- Radial tunnel syndrome. Carpal tunnel syndrome is a neurological disorder characterized by acute pain in the back of the hand and upper forearm that occurs when trying to move the fingers or wrist.
- Impaired supination of the hand and forearm. Supination of the hands and forearms is the ability to rotate the hand so that the palm faces down, parallel to the surface of the floor or thighs. With lesions of the radial nerve, impaired supination occurs quite often.
The symptoms of the disease vary depending on the location of the pathological process - it can be concentrated in the forearm, elbow or wrist.
For reference: one of the clear signs of pathology is the so-called “dropping hand” symptom (when trying to raise the arm up, the patient’s hand will hang down).
Radiation neuropathy refers to compression of nerves localized in the following areas of the extremities:
- Armpit – causes paralysis of the forearm muscles and weakening of the triceps muscle.
- Middle third of the shoulder.
- Elbow joint – this type of neuropathy is called “tennis player’s syndrome.” Damage to the nerve causes dystrophic changes in the ulnar ligaments and extensor muscles of the hand.
- Wrist.
The main symptoms of damage to the radial nerve, regardless of the cause of the damage, are approximately the same, and differ only in location.
Restoration of the radial nerve may be required for a patient after a fracture of the humerus, ulna or radius, carpal tunnel syndrome, diabetic angiopathy and a number of other diseases. Weakness of the muscles of the upper limb, a feeling of paresthesia and numbness of the skin, impaired motor skills of 1-3 fingers - all these are signs of damage to the radial nerve.
Finding and eliminating the potential cause is the primary stage of therapy. If the effect of the pathogenic factor is not eliminated, then starting a course of restorative therapy is useless. In the near future, an exacerbation will begin and the patient will return with the same symptoms.
To restore the radial nerve of the arm, different approaches can be used: medication, surgery, manual therapy, physiotherapy, etc.
In official medicine, drugs are most often used that improve the nutrition of the nerve fiber, stopping the inflammatory reaction at the site of supposed compression. This gives short-term results.
If serious obstacles are detected along the path of the radial nerve, restoration of its functional ability is possible through surgical intervention. During the operation, the doctor performs partial tissue resection.
These may be scar deformities that arise after injuries, inflammatory processes, etc. Also, conduction disturbances of the radial nerve are often associated with the growth of tumors. Fibromas, neuromas, atheromas, lipomas - all of them must be removed before the start of restorative therapy.
Complete treatment and restoration of the radial nerve of the hand is possible using manual therapy techniques. They allow not only to safely and effectively eliminate the cause of pathological changes, but also to start the processes of regeneration of damaged tissues.
Anatomy of the radial nerve: it consists of branches of the radicular nerves that arise from the 5th to 8th cervical vertebrae. It leaves the brachial plexus and passes through the axilla, heading along the lower dorsal surface of the arm to the hand.
In the area of exit from the armpit, it divides into several branches. Some of them are responsible for the performance of the muscles of the shoulder and forearm.
The other provides sensory abilities (skin sensitivity, determination of ambient temperature).
Physiology of the radial nerve: It consists of two types of axons. These are motor and sensory neurons. The first group is responsible for conducting a motor nerve impulse emanating from the structures of the brain to the muscles.
This is followed by a contractile reaction or relaxation of the myocytes. The second type of neurons is sensory or sensitive.
It collects data about interaction with the environment and transmits this information to brain structures for analysis and response.
Passage of the radial nerve along the upper limb:
- the ventral branches of the radicular nerves CV–CVIII enter the brachial plexus and exit from it on the other side;
- along the posterior surface of the axilla, the nerve descends along the subscapularis and latissimus dorsi muscles;
- in the anterior part of the armpit, the cutaneous nerve of the shoulder departs from it;
- along the groove of the radial nerve in the surface of the humerus passes to the elbow joint;
- passes along the brachioradialis muscle until it reaches the anterior surface of the forearm;
- along the brachialis muscle it passes to the capsule of the elbow joint and crosses it towards the supinator;
- there is a division into superficial and deep branches;
- the superficial branch enters the forearm and divides into five digital branches in the carpal tunnel region;
- the deep branch passes to the wrist joint and is responsible for the work of the flexor pollicis.
When affected at different levels, corresponding clinical symptoms may occur. An experienced neurologist who knows the anatomy and physiology of the radial nerve can easily make an initial diagnosis, which will then be confirmed during functional clinical diagnostics.
There are various causes of radial nerve damage. Most often at a young age these are various kinds of traumatic influences. Most often, the nerve is affected by stretching and tearing of the shoulder muscles. This may be a consequence of habitual dislocation or destruction of the labrum. Tunnel syndromes are in second place in terms of the prevalence of pathogenic factors.
Other causes of radial nerve damage include:
- osteochondrosis of the cervical spine and compression of the radicular nerves, complications of the disease, such as intervertebral disc herniation, protrusion, extrusion;
- instability of the position of the vertebral bodies, associated both with the development of osteochondrosis and with improper functioning of the tendon and ligamentous apparatus;
- vertebral subluxation;
- withers or hump formation in the area of the 6-7 cervical vertebrae;
- spondylosis and spondyloarthrosis;
- Ankylosing spondylitis, systemic lupus erythematosus, scleroderma and other rheumatoid and autoimmune processes in the human body;
- neck injuries;
- dislocations, fractures, sprains and tears in the upper shoulder girdle;
- lymphadenitis of the axillary group of lymph nodes;
- diabetic angiopathy and neuropathy;
- the impact of toxic substances on the human body (drinking alcoholic beverages, certain medications, smoking, working with salts of heavy metals);
- infections affecting bone and cartilage tissue (tuberculosis, polio, syphilis, etc.).
Among elderly patients, the leading cause of damage to the radial nerve remains deforming osteoarthritis of the shoulder, elbow and wrist joint. When they are destroyed and deformed, the nerve fiber is subject to inflammatory, edematous and traumatic effects.
Therefore, motor and sensory functions are quickly impaired. Severe, prolonged pain appears, which is replaced by muscle weakness and lack of skin sensitivity.
But in this case, neuropathy is often combined with damage to other nerve fibers, so the diagnosis is quite difficult to make; all possible diseases must be excluded.
It is necessary to begin restoration of the radial nerve after a fracture after the plaster cast is removed and the formation of a full callus is visible on the X-ray image. The course of restoration of the radial nerve after a fracture of the humerus is developed individually for each patient.
The doctor should pay attention to the possibility of the formation of a significant amount of scar tissue in the fracture area. There is also a risk of ankylosis and contracture of large and small joints. In this case, a functional decrease in the length of the nerve fiber occurs.
When trying to regain lost functions, acute pain occurs, which prevents full recovery.
To complete a recovery course, you must contact specialists. At home, without constant medical supervision, it is impossible to complete a full course of rehabilitation. There is a high probability of secondary damage to the nerve fiber and paralysis of the upper limb.
Restoration of the radial nerve after injury begins with a full functional diagnosis. Using special tests, an experienced neurologist will determine how affected the nerve structure is and in which areas of its passage compression is observed.
Then work will be carried out to eliminate the consequences of the injury. They usually consist in the fact that the soft tissues in the area of traumatic disruption of integrity are subject to scar deformation.
Functions
The radial nerve, innervating the above muscles, carries out motor functions, such as:
- supination of the hand,
- extension of the main phalanges of the fingers,
- extension in the wrist and elbow joints,
- abduction of the thumb.
The sensory fibers of the radial nerve are part of the nerves:
- posterior cutaneous nerve of the shoulder,
- posterior cutaneous nerve of the forearm,
- inferior lateral cutaneous nerve of the shoulder.
Sensitive fibers of the radial nerve innervate the skin on the radial side of the hand, the back surface of the shoulder and forearm, the dorsum of the first, second and part of the third finger of the hand.
Radial nerve injuries
Among the causes of the development of neuritis and plexopathies, the first place is occupied by injuries to peripheral nerves.
The upper extremities account for more than 40% of all peripheral nerve injuries.
The increase in the number of these neurological disorders is directly related to the increase in the number of injuries, which has been observed in recent decades, and is one of the most pressing problems of modern medicine.
Damage to peripheral nerves does not always manifest itself clinically - autonomic disorders, paresis, sensitivity disorders.
With an objective examination, in addition, it is difficult to assess the degree of nerve damage.
The result of delayed diagnosis is the involvement of peripheral nerves in the pathological process.
Further lack of necessary therapy can cause:
- nerve dysfunction (weakening muscle strength),
- sensory disorders, secretory and ischemic disorders),
- development of neurological syndromes that require long-term specialized treatment.
Neuropathy
Damage to the radial nerve occurs quite often. It can be damaged by squeezing or an awkward position of the hand during sleep, injury, or fracture. When walking for a long time on crutches and during compression with hooks during operations. Disruption of innervation can also be observed due to compression by a tumor extending from neighboring tissue. Malignancy is extremely rare in this location.
According to medical data, radial neuritis is the most common pathology of the upper extremities. The causes of radial neuritis depend on many factors.