general description
Damage to the external (lateral) popliteal nerve (G57.3) is a neuropathy of the peroneal nerve, manifested by muscle weakness and decreased sensitivity of the lateral part of the leg.
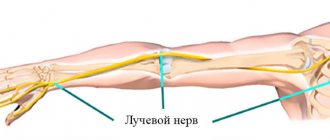
| Peroneal nerve 1 - sciatic nerve, 2 - peroneal nerve, 3 - musculocutaneous nerve, 4 - deep peroneal nerve, 5 - neck of the fibula, 6 - biceps femoris muscle, 7 - peroneus longus muscle |
More common between the ages of 40–60 years. The nature of the lesion is unilateral.
In most cases, the cause of the lesion is a lower leg injury. Less commonly, the lateral popliteal nerve is damaged by injury to the knee/ankle joint, compression of the leg during sleep, tight casting of the lower leg, or prolonged squatting.
Diagnosis of the disease
To identify pinched sciatic, femoral or tibial nerves, it is necessary to determine the cause of the disease.
The diagnosis is made by a neurologist using a combination of several diagnostic methods:
- External examination and questioning of the patient about the initial signs of the disease.
- X-ray examination in various projections.
- MRI of the knee or lower back including the lower extremities.
- Study of the conductivity of nerve endings using electrical impulses.
- Electromyography.
- Lasegue test (“tension symptom”). The study is characterized by raising the straightened leg in order to identify the pinched area. The test is positive if you feel severe pain in the lower back or hip joint.
- Lerrey's symptoms. To detect signs of inflammation in the nerves, the patient is asked to rise from a lying position.
- Bekhterev's method - when raising a healthy leg, pain appears in the affected limb.
Additionally, consultation with an oncologist, rheumatologist or neurosurgeon is prescribed.
Clinical picture
The disease manifests itself as weakness in the leg, pain in the lower leg/foot area is less common. Numbness gradually appears in the back of the foot and the lateral surface of the lower leg. Patients may complain of burning, tingling in the lower leg/foot.
An objective examination of the patient reveals pain on palpation in the area of the head of the fibulae (80%), hypoesthesia of the dorsum of the foot (70%), hypoesthesia/analgesia of the lateral surface of the leg (65%), weakness in the extensors of the foot and fingers (75%), muscle atrophy on shins (70%). Plantar flexion with foot supination causes/increases pain in the head of the fibulae (85%). Walking on your heels is difficult or impossible (50%). Paresthesia is detected in the foot (20%).
Symptoms
Signs vary depending on the nature of the lesion and its level. For example, with a complex injury (fracture), all signs appear immediately, but may not be noticeable due to other injuries. If the cause is a less visible and tangible factor, then the signs will appear subtly and gradually.
Symptoms can be divided into two groups:
- sensitive;
- motor.
If this nerve is damaged, it is diagnosed:
- sensory disturbance;
- pain that gets worse if you squat;
- difficulty in straightening the foot;
- weakness;
- unable to walk on heels;
- walking disorder;
- deformation of the foot (drops and rolls down);
- the leg is losing weight.
If the problem is not corrected, the muscles begin to atrophy, which leads to serious impairments in a person’s functional capabilities.
Treatment of damage to the external (lateral) popliteal nerve
Treatment is prescribed only after confirmation of the diagnosis by a medical specialist. Symptomatic treatment is carried out (decongestants, analgesics, vitamins), physiotherapy, massage, novocaine and hydrocortisone blockades are indicated.
Essential drugs
There are contraindications. Specialist consultation is required.
- Voltaren (non-steroidal anti-inflammatory drug). Dosage regimen: IM at a dose of 75 mg (contents of 1 ampoule) 1 time/day.
- Ketoprofen (non-steroidal anti-inflammatory drug). Dosage regimen: IM - 100 mg 1-2 times a day; after pain relief, it is prescribed orally in a daily dose of 300 mg in 2-3 doses, a maintenance dose of 150-200 mg/day.
- Tramadol (analgesic). Dosage regimen: IV, IM, SC in a single dose of 50-100 mg, possible repeated administration of the drug after 4-6 hours. The maximum daily dose is 400 mg.
- Diacarb (diuretic). Dosage regimen: 0.25 g orally 2 times a day (morning, afternoon) for 5-7 days.
- Milgamma (B complex of vitamins). Dosage regimen: therapy begins with 2 ml intramuscularly 1 time per day for 5-10 days. Maintenance therapy - 2 ml IM two or three times a week.
Treatment of a pinched nerve
Before starting therapy, it is necessary to determine what specific disease affected the pinched nerve of the knee joint and eliminate the cause.
Treatment is carried out using:
- conservative remedies;
- physiotherapy;
- exercise therapy;
- acupuncture.
Massage and manual therapy sessions are not indicated for all diseases. Sometimes these methods can seriously impair the healing process of a pinched nerve.
In advanced cases or when tumors are removed, surgery is used.
The first step is to relieve pain and inflammation:
- To relieve pain, a person should remain in bed and not subject the injured limb to stress. Rubbing in anti-inflammatory agents for external use (Ketonal, Fastum gel) helps well. If the desired effect does not occur, then the pain is relieved with analgesic drugs or injections.
- The inflammatory process is eliminated using NSAIDs or hormonal blockades.
- Muscle relaxants and antispasmodics will help relieve nervous tics.
- To restore blood circulation and tissue nutrition, injections with vitamins are indicated.
Incidence (per 100,000 people)
| Men | Women | |||||||||||||
| Age, years | 0-1 | 1-3 | 3-14 | 14-25 | 25-40 | 40-60 | 60 + | 0-1 | 1-3 | 3-14 | 14-25 | 25-40 | 40-60 | 60 + |
| Number of sick people | 0 | 0 | 0 | 4.4 | 6.5 | 8.6 | 5.2 | 0 | 0 | 0 | 4.4 | 6.5 | 8.6 | 5.2 |
Prevention
You can prevent recurrence of a pinched nerve by following the rules:
- You need to sleep on a hard, flat surface.
- Avoid heavy lifting and excessive physical activity.
- Do not make quick turns or sudden movements.
- Avoid hypothermia of the extremities and lower back.
- Lose weight, try to adjust your diet and eliminate salted fish, smoked foods, alcohol and caffeine.
- Every morning, do special exercises or just take a walk in the park.
- Swimming has a general strengthening effect on the body.
- Constantly monitor your posture.
A pinched nerve is an unpleasant disease that causes discomfort and pain. If you consult a doctor in a timely manner and identify the cause, the disease goes away faster, and the person returns to the usual rhythm of life without pain.
Consequences and complications
The consequences of injuries to the median nerve can be very serious: all three types (neuritis, neuropathy, neuralgia) are classified as common and severe, which in advanced cases lead to complete or partial disability.
With insufficient treatment, or in the absence of it, the sick person is forced to change his profession and lifestyle.
There are frequent cases of disability due to atrophy of the muscle tissue innervated by the affected nerve. Unfortunately, at present, a significant number of errors are often made both in the diagnosis and in the treatment of this pathology.
Symptoms of neuritis of the axillary nerve
The nature and severity of the lesion largely depends on which fibers of the axillary nerve were damaged: in its body there are motor, sensory and autonomic fibers. Each type of lesion is characterized by a different pattern of damage:
- damage to motor fibers - complete or partial decrease in strength and tone in the muscles innervated by the inflamed nerve, muscle atrophy, impaired tendon reflexes of varying severity;
- damage to sensory fibers - numbness, paresthesia, weakening of sensitivity in the affected area;
- inflammation of vegetative fibers - swelling, cyanosis of the skin, local hair loss or loss of hair color, the skin in the innervated area becomes dry and thin, nails become brittle, trophic ulcers form, etc.
The primary symptoms of inflammation of the peripheral nerves in most cases are numbness and pain. Also, in each specific case, specific symptoms may appear, depending on the functional purpose of the area innervated by the affected nerve.
Neuritis of the axillary nerve is accompanied by difficulty or inability to raise the arm to the side, weakened sensitivity in the first third of the shoulder area, decreased tone or complete atrophy of the deltoid muscle, and increased mobility of the shoulder joint.
Provoking factors
Morton's neuroma develops under the influence of certain external and internal factors. Among the most common reasons are the following:
- Overweight . This reason is the most common, since excess pressure is constantly placed on the lower extremities and nerves are regularly compressed, which leads to the development of Morton's neuralgia.
- Injuries and bruises of various types.
- Infectious diseases that have become chronic are also negatively reflected .
- Flat feet . Many people mistakenly believe that this pathology does not entail serious consequences, but it is the initial stage of many serious diseases. Morton's disease is one of them.
- Regularly wearing shoes with long heels . This in turn leads to bone deformation. Nerve inflammation is one of the consequences.
- Tight shoes . When it is constantly worn, compression of the nerve fibers occurs. This may be accompanied by constant pain and neuralgia.
- Foot tumor.
- Leg overload . When standing for a long time, the feet experience unnatural overloads, which lead to many different diseases.
High heels and uncomfortable shoes are a direct path to plantar neuralgia
Causes of tibial nerve neuropathy
The most common cause of tibial nerve neuropathy is its injury as a result of a number of pathological factors:
- In the first place among all causes are injuries (fracture, bruise, dislocation) of the lower leg, foot, ankle joint or their consequences.
- Chronic microtraumatization (long-term exposure) to increased stress on the nerve in athletes and workers with professional loads on the ankle joint.
- Pathological changes in the ankle joint, which leads to narrowing of the canal and compression of the nerve passing through it. Occurs in arthrosis, dislocations, arthritis and other conditions.
- Heredity. Increased vulnerability of nerve fibers or hereditary narrowness of the canals in which the tibial nerve passes.
- Hormonal disorders (diabetes mellitus, hypothyroidism, postpartum period, pregnancy).
What provokes the destructive process
There can be many reasons for damage to the median popliteal nerve; in addition to the common ones - trauma, inflammation, compression, the following can be distinguished:
- slow blood circulation due to varicose veins;
- valgus flatfoot;
- rheumatoid arthritis;
- prolonged sitting cross-legged;
- wearing excessively tight shoes;
- changes in the musculoskeletal system
- reflex muscular-tonic disorders due to spinal curvature (osteochondrosis, scoliosis, spondyloarthrosis);
- surgical interventions resulting in incorrect positioning of the leg;
- diseases resulting in proliferation of connective tissue (gout, polymyositis);
- metabolic disorders (diabetes mellitus, obesity);
- intoxication (alcohol, drugs);
- local tumor processes.
Article on the topic: Risk factors for hypertension - endogenous and related to lifestyle, environmental influences
Types of nerve damage
Damage to the median popliteal nerve is not so common due to its location, and usually occurs in pre- or retirement age (up to 60 years) in persons suffering from inflammatory processes localized in the lumbosacral region, in persons with a chronic form of recurrent sciatica, Athletes often suffer from it.
The etiology of the development of pathology in the popliteal part of the tibial nerve is primarily associated with the following factors:
- injury;
- inflammation;
- toxic effects, deformation, compression, etc.
There are three types of median nerve injury:
- neuralgia;
- neuritis;
- neuropathy.
More details about each type of damage:
All processes differ from each other in etiology, course, treatment methods, and consequences.
TIBIAL NERVE NEUROPATHY
The tibial nerve is a continuation of the sciatic nerve. It crosses the popliteal fossa from top to bottom, giving branches at this level to the triceps surae muscle, long flexor muscles of the fingers and thumb, tibialis posterior, popliteal and plantar muscles. The internal cutaneous nerve of the leg also departs here, which, after exiting under the skin, anastomoses with the branches of the peroneal nerve in the lower third of the leg and forms the sural nerve, innervating the ankle joint and the skin of the posteroexternal surface of the lower third of the leg, the heel and the outer edge of the foot to the nail phalanx of the fifth toe. From the main trunk of the tibial nerve, in addition to the muscle branches, depart the interosseous nerve, articular branches to the knee and ankle joints, internal calcaneal nerves, which, perforating the fascia, scatter in the skin of the posterior-internal part of the heel and sole. Next, the nerve, together with the posterior tibial artery, enters the tarsal canal in its posterior compartment outward from the tendon of the long flexor of the big toe; here the nerve and artery are fixed by a powerful internal annular ligament - the flexor holder. At this point, the nerve can be palpated midway from the posterior edge of the medial malleolus to the Achilles tendon. Upon exiting the canal, the tibial nerve divides into the internal and external plantar nerves. The medial plantar nerve (analogous to the median nerve) innervates the muscles of the eminence of the big toe, the skin of the medial edge of the sole of the foot, the corresponding three and a half toes on the plantar and their nail phalanges on the dorsum of the foot. The lateral part of the sole and the remaining one and a half toes on the plantar surface, as well as their nail phalanges, are completely supplied by the lateral plantar nerve. It also provides innervation to all the remaining small muscles of the foot (by analogy with the ulnar nerve).
Damage to the tibial nerve in the popliteal fossa leads to atrophy of the posterior muscles of the leg and small muscles of the foot; in this case, plantar flexion of the foot is impaired (it takes the shape of a heel foot). The patient walks, leaning on his heel, cannot step on his toe, and there is no movement of the fingers. Damage to the nerve in the lower leg and in the tarsal canal leads to atrophy of the small muscles of the foot, which takes on the appearance of a “clawed foot.” High compression of the nerve before the origin of the medial cutaneous nerve of the leg is accompanied by sensitivity disorders on the back surface of the leg, on the lateral surface of the lower third of the leg and foot, as well as on the heel and on the plantar surface of the foot. Isolated sensory disturbances on the sole and toes and severe pain syndrome occur with compression of the nerve in the tarsal canal and with damage to the plantar nerves. Causalgic syndrome with severe vegetative-vascular and trophic disorders of the foot, osteoporosis of the foot bones, edema, hyperpathia is typical for traumatic injuries of the tibial nerve and its branches at different levels.
High compression-ischemic neuropathy, features of the clinical picture, etiopathogenetic factors - see “Politeal syndrome”. Let us recall that in this case a combined lesion of the tibial and peroneal nerves often occurs.
Tarsal tunnel syndrome. The tibial nerve is most often subject to compression at the level of the ankle joint. The predominant cases are vertebrogenic tunnel lesions associated with stenosis of the tarsal canal due to neurodystrophic changes in the ligaments, tendons and bone structures of the corresponding ankle joint. A variety of predisposing factors include fibrous post-traumatic changes in the canal area, tenosynovitis, ganglion, fat pad in obesity, hypertrophy or abnormal location of the adductor pollicis muscle, flat feet, and varus deformity of the foot. The onset of symptoms may be triggered by running or long walking.
Patients complain of burning pain, numbness in the area of the plantar surface of the foot along its lateral or medial edge. As a rule, the pain spreads to the calf muscle; it is dull, deep, intensifies when standing and walking. Sometimes hypoesthesia is determined along the medial or lateral edge of the sole. Movement in the ankle joint is full, there is no paresis of the foot. Minimal weakness of the small muscles of the foot is manifested by its flattening and slight clawing of the toes. The Achilles reflex is preserved. Percussion of the nerve through the flexor holder at the level of the canal or at the edge of the scaphoid at the exit from the tarsal canal increases pain and causes paresthesia.
Neuropathy of the internal plantar nerve is the result of compression and repeated traumatization in the canal between the plantar aponeurosis and the head of the abductor pollicis muscle. Pain and paresthesia are localized along the medial edge of the foot on the sole, in the big toe and in one or two adjacent toes. The pain point is determined on the medial surface of the foot behind the tuberosity of the navicular bone; its percussion provokes a burning pain in the thumb. This syndrome is typical for long-distance runners and people involved in recreational running.
Plantar neuropathy of the common digital nerves (Morton's metatarsal neuralgia). The syndrome is associated with chronic trauma to the plantar common digital nerves in the spaces between the heads of the third and fourth, and less commonly, the second and third metatarsal bones. Usually older, overweight women who wear high-heeled shoes and begin to jog and walk a lot are affected. Pain from the arch of the foot and the balls at the base of the toes spreads to their tips and sharply intensifies when standing, running and walking. The examination reveals painful points between the heads of the metatarsal bones, increased burning pain in the fingers; Tinel's sign is positive. Sensitivity in the second and third interdigital spaces may be reduced. Rest and changing shoes relieve pain.
Median nerve neuropathy
Affected nerve endings lead to disruption of the transmission of impulses from the central nervous system to muscle tissue and organs. Because of this, sensitivity, motor, and trophic functions change. Neuropathy may manifest as:
- numbness of the limb;
- tingling, burning;
- spasmodic pain when moving;
- weakness, low muscle tone, atrophy.
Treatment of neuropathy is aimed primarily at eliminating the consequences: in case of wounds and injuries, plastic surgery is performed, the nerve is sutured, tumor formations are also surgically removed, and at the same time pain is relieved.
In general, therapy for median nerve neuropathy is long-term, so the course of treatment is complex and includes:
- medications (B vitamins, metabolic drugs, NSAIDs);
- physiotherapeutic (electrophoresis, magnetic therapy, massage, physical therapy, etc.);
Treatment of neuritis of the axillary nerve
The main goal of treatment for neuritis of this nerve is to eliminate the cause of its occurrence. Therefore, first of all, the doctor must determine what problem provoked the inflammation of the peripheral nerve:
- If the cause is an infectious disease, then the patient should be prescribed antibacterial or antiviral drugs - the doctor will make the exact prescription after receiving the results of the relevant tests.
- In situations where the development of neuritis is provoked by disturbances in the functioning of the cardiovascular system, vasodilator drugs are prescribed.
- To cure neuritis of a traumatic nature, it is necessary to ensure complete immobilization of the injured limb.
If inflammation of the axillary nerve is caused by compression by crutches, then the patient should replace them with other means of similar use during recovery. If it is not possible to find such a replacement, the use of crutches should be minimized. In a situation where the disease is caused by a dislocation of the humerus, it is necessary to completely immobilize the injured area until the inflammatory process is completely relieved.
Next, anti-inflammatory drugs, B vitamins, analgesics, and decongestants are used. After a 2-week course of treatment, anticholinesterase medications and stimulants of biogenic processes are additionally prescribed.
A properly selected course of physiotherapy, which is added to the treatment plan from the end of the first week, is also of great importance for the successful treatment of neuritis. Among the methods of physiotherapy that are most effective in the treatment of neuritis are:
- electrophoresis with various drugs;
- ultraphonophoresis;
- impulse currents;
- UHF.
In addition, medical massages and exercise therapy can effectively and quickly normalize the functions of the affected area. Electrical stimulation is used to restore sensitivity and tone of damaged muscles. If neuritis due to a narrow musculoskeletal canal has taken the form of tunnel syndrome, then methods of direct injection of medications are used.
Characteristic symptoms
A characteristic feature of nerve compression in the knee joint is pronounced symptoms, which can manifest not only in the knee area, but throughout the entire length of the nerve.
The main symptoms of a pinched nerve include:
- severe, sharp pain that intensifies with movement or while fixing a limb in a certain position;
- pain when pressed, as the inflamed nerve becomes very sensitive to any external influences;
- loss of full mobility of the limb, in particular, problems arise when moving the leg to the side or bending the knee;
- numbness of the leg caused by deterioration in the conduction of nerve impulses of the damaged nerve;
- a nervous tic or involuntary jerking of a limb is associated with compression of the sciatic nerve, which most often occurs during pregnancy.
Establishing diagnosis
Diagnosis is carried out taking into account clinical and neurological data. In order to correctly diagnose a lesion, the following sequence of methods is used:
- Survey (about the state, activity of uncomfortable sensations).
- Palpation to identify compactions.
- Examination to identify the muscle-trunk symptom of Lasègue. When walking, patients tend to limp on the side that is damaged due to its imaginary shortening. This symptom in most patients can even be detected several years after the first symptoms appear.
- Due to similar manifestations of vertebrogenic pathology, doctors practice examining the spine and knee joint using radiography.
- Additionally, the nature of the damage is revealed using ultrasound diagnostics, MRI, and electromyography.
Patellar tendon pain
It is not uncommon to experience pain in the tendon above the knee. The main cause of such pain is a tear of the meniscus after a strong blow or fall on the anterior region of the kneecap. New pain may indicate ligament damage or disruption of the integrity of the periarticular cartilage.
The cause of acute pain above the knee can be arthrosis, in which inflammation and infection begin to appear in the joint cup. Prolonged exercise can also be a culprit for patellar tendon pain. For people with an active lifestyle who play sports, prolonged exercise can cause inflammation and further rupture of the ligaments. In this case, it is necessary to give the joints a rest in time and apply a special pad to the kneecap that fixes the ligaments and tendons in the correct position.
Most often, pain after intense physical activity appears above the knee in the evening or in the morning of the next day. The main symptoms of sprained ligaments and tendons are difficulty in moving the legs, the appearance of edema, swelling and blue discoloration. In this case, special fixing bandages will not be enough for effective treatment; the doctor will prescribe ointments, as well as painkillers. A torn meniscus will require emergency knee surgery.
Pain in the patellar tendon can occur when the integrity of the cartilage is damaged, which is caused by:
- High physical activity;
- Excess body weight;
- Arthrosis;
- Poor circulation;
- Sedentary lifestyle;
- Lack of minerals in the body that are responsible for the condition of bone and cartilage tissue;
- Previous injuries to the knee joint.
Based on what cause the doctor determines after complete diagnosis, a specific treatment will be prescribed. It consists of physiotherapeutic procedures, for example, electrophoresis, magnetic therapy or ultrasound, and is also supplemented by therapeutic massages, medications, selection of proper nutrition, vitamins and minerals. During treatment and during the rehabilitation period, it is necessary to completely avoid physical activity on the knee joint.