The inflammatory process that begins in the brain has a fairly acute course and many consequences. Among the varieties of this group of diseases one can distinguish inflammation of the arachnoid mater (arachnoiditis). This type of disease belongs to the group of serous inflammatory processes and is characterized by impaired blood circulation and weakening of capillary walls. This phenomenon leads to the fact that lymph leaks from the vessels into the soft tissues and stagnation occurs in them. Swelling gradually develops, the temperature rises and other meningeal symptoms occur.
What is myelitis
Inflammatory processes in the brain tissue of the spine, regardless of location and catalyst, are called myelitis. Types of inflammation are classified as follows:
- According to etiology.
- Localizations.
- The course of the disease.
The most common is transverse myelitis of the spinal cord. With this diagnosis, focal localized inflammation is observed that disrupts the integrity of the brain tissue. Inflammatory processes affecting all parts of the spine are rare.
Causes of myelitis
Inflammation of the brain can be caused by many reasons.
It is customary to classify myelitis depending on the catalysts into the following groups: In addition to the above reasons, myelitis can be provoked by any disease that suppresses the human immune system and destroys the membrane of nerve cells.
Classification by development and etiology of inflammation
Myelitis is classified into several groups, depending on the intensity of spread, course of the disease, and etiology.
Spinal cord inflammatory syndromes
As a rule, the development of the disease is preceded by a prodromal period.
At this time, it is possible to identify the symptoms of inflammation and prescribe the most effective treatment. During the prodromal period, the patient experiences:
- Weakness.
- Muscle pain.
- Increase in body temperature to 38-39°C.
- General weakness and malaise.
Further symptoms of the lesion depend on the location and type of the inflammatory process:
- Acute transverse myelitis - characterized by pain at the site of the lesion, paresthesia of the lower extremities, unpleasant sensations in the form of numbness, tingling, etc. As the disease progresses, urinary function disorders and fecal retention are observed. It is important to prescribe timely therapy, since acute transverse myelitis is an inflammation of the spinal cord leading to paralysis.
- Acute disseminated myelitis - inflammatory processes are “scattered” across different levels of the spinal cord. As a result, the intensity of the lesion is slightly lower compared to focal inflammation. The remaining symptoms remain the same as those of the previous disease.
- Subacute necrotizing myelitis - numbness, sensory disturbances, partial or complete paralysis of the limbs are observed. The levels of spinal cord damage are always higher than the area of symptoms.
According to statistics, damage to the spinal cord in the lumbar and sacral region is extremely rare. The inflammatory process occurs at the level of the cervical and thoracic spine.
Symptoms of arachnoiditis[edit | edit code]
The disease develops subacutely with the transition to a chronic form. Clinical manifestations are a combination of general cerebral disorders, more often associated with intracranial hypertension, less often with liquor hypotension, and symptoms reflecting the predominant localization of the meningeal process. Depending on the predominance of general or local symptoms, the first manifestations may be different.
Among the general cerebral symptoms, headache is common, most intense in the early morning hours and sometimes accompanied by nausea and vomiting. The headache can be local, aggravated by straining, straining or awkward movement with firm support on the heels (a symptom of jumping is a local headache when jumping with an unabsorbed descent on the heels).
Focal symptoms depend on the location of arachnoiditis. Convexital arachnoiditis is characterized for the most part by a predominance of the phenomena of brain irritation over signs of loss of function. One of the leading symptoms is generalized and Jacksonian epileptic seizures. With basal arachnoiditis, general cerebral symptoms and dysfunction of the nerves located at the base of the skull are observed.
A decrease in acuity and changes in visual fields can be detected with opticochiasmatic arachnoiditis. Clinical manifestations and fundus images may resemble symptoms of optic neuritis. These manifestations are often accompanied by symptoms of autonomic dysfunction: severe dermographism, increased pilomotor reflex, profuse sweating, acrocyanosis, sometimes thirst, increased urination, hyperglycemia, adiposogenital obesity.
In some cases, a decrease in sense of smell may be detected. Arachnoiditis in the area of the cerebral peduncles is characterized by the appearance of pyramidal symptoms, signs of damage to the oculomotor nerves, and meningeal signs. With arachnoiditis of the cerebellopontine angle, headaches in the occipital region, noise in the ear and paroxysmal dizziness, and sometimes vomiting occur.
Symptoms of damage to the auditory, trigeminal, abducens and facial nerves may be observed. Arachnoiditis of the large (occipital) cistern develops acutely, the temperature rises, vomiting, pain in the back of the head and neck appears, aggravated by turning the head, sudden movements and coughing; damage to the cranial nerves (IX, X, XII pairs), nystagmus, increased tendon reflexes, pyramidal and meningeal symptoms.
With arachnoiditis of the posterior cranial fossa, damage to the V, VI, VII, VIII pairs of cranial nerves is possible. Intracranial hypertension, cerebellar and pyramidal symptoms are often observed. Differential diagnosis with tumors of the posterior cranial fossa is mandatory. Lumbar puncture is performed only in the absence of congestion in the fundus.
What happens if the spinal cord is inflamed?
Dysfunction of the spinal cord immediately affects the capabilities of the human body.
The development of the inflammatory process leads to movement disorders, numbness and paralysis of the limbs, and other unpleasant complications. The progression of the disease leads to the spread of the inflammatory process down to the lower part of the brain. The syndrome of complete transverse spinal cord lesions retains symptoms throughout the patient's life, and no deterioration in well-being is observed.
A favorable treatment prognosis depends on early diagnosis of the disease and timely prescribed therapy.
Features of inflammation in the nerve roots
The most common form of inflammation of the spinal cord is damage to the spinal nerve roots or radiculitis. The pathology can be localized in the cervical, thoracic and most often in the lumbar region, which bears a very heavy load. The reasons for the development of the inflammatory process in the roots of the spinal nerves are as follows:
- backbreaking, hard physical labor;
- osteochondrosis of all parts of the spine;
- hernia;
- erasing disks.
Often the inflammatory process of the spinal nerve becomes chronic. If symptoms appear in the form of sharp pain in the sacral area and movement disturbances, the nerve endings are most likely pinched. Treatment in most cases consists of complete rest and strict bed rest. Warming ointments or patches relieve pain well.
Sometimes during acute pathology of the roots, a drug blockade is needed.
If the disease has become chronic, it is necessary to perform special physical exercises and massage. The causes of inflammation of the spinal nerve roots are as follows:
- severe hypothermia of the body;
- damage to one or all parts of the spine due to trauma;
- lack of vitamins and minerals, especially lack of calcium and impaired metabolism;
- frequent stressful situations;
- various infectious diseases.
All these factors can trigger a painful attack and other symptoms. A common form of damage to the spinal nerve roots is inflammation in the lumbar region. A small percentage is due to infectious meningoradiculitis, where the infection spreads to the membranes of the brain and a cerebrospinal fluid test will be required to make a correct diagnosis.
How to treat spinal cord myelitis
Treatment of inflammation requires mandatory hospitalization of the patient.
The course of therapy depends on the patient’s condition and the results of differential diagnosis of inflammatory lesions of the spinal cord. Treatment of the inflammatory process includes the following:
What medications are used
When prescribing medications, the patient’s general condition, the presence of allergic reactions and contraindications are taken into account.
Prednisolone is traditionally used as a medicine for inflammation. Injections continue to be given until the patient feels better. Furosemide and Mannitol are prescribed as diuretics. Since with myelitis of the thoracic, cervical and lumbar spinal cord there is a deterioration in the blood supply, bedsores must be prevented. Analgesics and antibiotics are prescribed individually.
Spinal cord meningitis: serous form
The development of the serous form of spinal cord meningitis is similar to the development of purulent spinal meningitis. The occurrence of this pathology is caused by Koch's bacillus, enteroviruses, and Coxsackie virus disease.
Serous meningitis of the spinal cord is manifested by the following symptoms:
- headaches and other constant pain;
- significant increase in body temperature;
- feeling of weakness;
- drowsiness;
- diarrhea and vomiting;
- stiffness of the neck muscles;
- difficult tolerance to noise effects, photosensitivity;
- difficulties in flexing and straightening limbs;
- the appearance of skin rashes;
- development of conjunctivitis.
An important symptom of the serous form of spinal meningitis is severe pain in the head. Such pain makes it difficult to tilt the head towards the neck or turn it to the side, as a result of which the patient is forced to constantly be in a lying position.
The disease progresses very quickly. For example, a person who feels fine in the morning may find himself unable to perform simple movements by lunchtime. Like purulent meningitis, serous spinal meningitis can lead to a significant deterioration of the patient's condition, including coma.
To identify the serous form of meningitis of the spinal cord, specialists at the Yusupov Hospital prescribe a lumbar puncture, which allows one to examine the cerebrospinal fluid for the presence and number of lymphocytes.
Rehabilitation after myelitis
Rehabilitation of people with infectious lesions of the spinal cord allows partial or complete restoration of motor functions lost as a result of inflammation.
During hospitalization, bedsores are prevented. The doctor assesses the patient's general condition and the extent of the lesion. After this, effective neurorehabilitation is prescribed, including:
- Visit to a psychologist.
- Social adaptation.
- Physiotherapy and massage.
Timely rehabilitation allows you to completely restore lost mobility and other body functions.
Most adults suffered from many infectious diseases in childhood: chicken pox, measles, rubella, mumps. At the present stage of development of medicine, the strategy of using vaccine prophylaxis as an effective method of preventing the above diseases is dominant. These measures will allow you to avoid many serious complications, one of which is spinal cord myelitis.
The spinal cord is the second most important outpost of the central nervous system after the brain. The organ is located inside the cavity formed by the vertebrae and consists of a combination of gray and white matter. The first anatomical formation is a collection of neuron bodies (nerve tissue cells), the second is their processes. The former are responsible for the movement of skeletal muscles and maintaining their tone, the latter are responsible for conducting an electrical signal (nerve impulse) to the brain and in the opposite direction. A cross section of the spinal cord resembles a butterfly in appearance. The spinal cord, by analogy with the spine, is divided into a number of sections: cervical, thoracic, lumbar, sacral. In the first and third there are centers for controlling the motor functions of the muscles of the limbs.
Anatomical structure of the spinal cord
Myelitis is a medical term for inflammation of the spinal cord.
Synonyms for the disease: inflammation of the spinal cord, spinal myelitis.
The pathology occurs with a frequency of no more than five cases per million population.
It is not possible to identify risk groups for the development of myelitis. The process equally often affects people of different genders and ages.
Classification
- According to the localization of the inflammatory process, the disease is divided into:
- Based on the reason that caused the pathological process, myelitis is divided into: traumatic, in which the disease begins with mechanical damage to the spine and spinal cord;
- autoimmune, which is based on the damaging effect of one’s own immune mechanisms on the spinal cord tissue;
- infectious, in which the inflammatory process of the spinal cord is based on the pathogenic action of bacteria (causative agents of meningitis, syphilis, tuberculosis) or viruses (causative agents of herpes, intestinal infections, HIV);
- post-radiation, which is based on the pathological effects of radiation (ionizing radiation);
- intoxication, in which toxic substances (medicines, harmful production factors) have a damaging effect on nerve cells;
- primary, in which the pathological process begins with damage to the nervous system (meningitis, poliomyelitis);
- acute stage, in which symptoms characteristic of other pathologies accompanied by inflammation predominate;
Infectious agents are the cause of spinal cord myelitis
Meningococcus - the causative agent of meningitis Treponema pallidum - the causative agent of syphilis Poliovirus - the causative agent of poliomyelitis HIV virus - the causative agent of human acquired immune syndrome Mycobacterium tuberculosis - the causative agent of tuberculosis
Poliomyelitis virus is one of the causes of inflammation of the spinal cord - video
Causes and factors for the development of the disease
The primary link in the development of the inflammatory process is the action of a damaging factor - trauma, infectious, toxic agents, the pathological influence of one’s own immune mechanisms. The consequence is the formation of edema of the spinal cord tissue. An increase in the volume of an organ located in a closed space of the spinal canal triggers a violation of its blood circulation, as well as the formation of small blood clots in the vessels - thrombi. Lack of blood supply inevitably leads to disruption of the structure of the spinal cord, its softening, and the death of some areas. In the area where the former focus of inflammation is located, a scar is formed that does not have the specific properties of spinal cord cells, as a result of which a disruption in its functioning is observed.
Predisposing factors include:
Clinical picture of the disease
In different groups of patients, including pregnant women, newborns and infants, the pathological process in the substance of the spinal cord occurs with a similar clinical picture.
Differences in neurological manifestations in spinal cord myelitis of different localizations
Optico-chiasmatic arachnoiditis[edit | edit code]
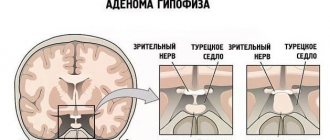
Arachnoiditis of the base of the brain is more common. The most common location is the chiasmatic region, which is the reason for the relative frequency of opto-chiasmatic arachnoiditis. The importance of studying this form is determined by the involvement of the optic nerves and the area of their decussation in the process, which often leads to irreversible loss of vision.
In the area of the chiasm and intracranial part of the optic nerves, multiple adhesions and cysts form in arachnoiditis. In severe cases, a scar membrane is created around the chiasm. As a rule, opticochiasmatic arachnoiditis is not strictly local: less intense changes are also found at a distance from the main focus.
The optic nerves in opticochiasmatic arachnoiditis are affected by mechanical factors (compression of adhesions), as well as the transition to their myelin sheath of the inflammatory process and circulatory disorders.
Opticochiasmatic arachnoiditis usually develops slowly. First, arachnoiditis affects one eye, then gradually (over several weeks or months) the other is also involved. The slow and often unilateral development of opticochiasmatic arachnoiditis helps differentiate the process from retrobulbar neuritis.
The degree of vision loss in opticochiasmatic arachnoiditis can be different - from decreased vision to complete blindness. Often, at the onset of the disease with opto-chiasmatic arachnoiditis, there is pain posterior to the eyeballs. The most important aid in the diagnosis of opto-chiasmal arachnoiditis is the study of the visual fields and fundus.
From the fundus of the eye, in 60-65% of cases, atrophy of the optic nerves (primary or secondary, complete or partial) is determined. In 10-13% of patients, congestive papillae of the optic nerve are found. Manifestations from the hypothalamic region are usually absent. An image of the sella turcica also does not reveal pathology.
Arachnoiditis of the meninges is a consequence of previous injuries or concomitant infectious diseases of the brain and paranasal sinuses.
Diagnostic methods
To establish a diagnosis of spinal cord myelitis, the following measures are used:
Knee Reflex Diagram
Spinal puncture (lumbar puncture) is the most important method for diagnosing spinal cord myelitis
Electroneuromyography is one of the components of diagnosing spinal cord myelitis
Tomographic image of the focus of inflammation of the spinal cord
Differential diagnosis is carried out with the following diseases:
Myelitis
Myelitis
– a general name for any inflammatory processes of the spinal cord. Symptoms directly depend on the level and extent of the lesion; most often it is pain (its irradiation), paralysis, pelvic dysfunction, sensory disturbance and others.
Diagnosis of myelitis includes a neurological examination and assessment of the parameters of cerebrospinal fluid taken for analysis by lumbar puncture. CT or MRI of the spinal cord and myelography may also be prescribed.
Treatment includes the prescription of antibiotics, anti-inflammatory drugs, analgesics, muscle relaxants, as well as exercise therapy, massage and physiotherapeutic procedures.
Myelitis is the general name for all inflammations of the spinal cord that can affect both gray and white matter. That is, myelitis is any spinal inflammatory process.
This disease can hardly be called widespread; it occurs in no more than 5 cases per 1 million people.
It is impossible to identify any features in the structure of the incidence of myelitis; gender or age have virtually no effect on the risk of developing the disease. Some researchers provide evidence that myelitis most often affects people aged 10 to 20 years and the elderly.
Sometimes it is not possible to accurately establish the cause of the development of myelitis, but in most cases, the main “trigger factors” are still known.
The only classification of myelitis used in clinical neurology is based precisely on etiology, that is, the cause of its occurrence.
According to this classification, three variants of the disease are distinguished: infectious, traumatic and intoxication.
Infectious myelitis
. Accounts for almost half of all cases. This type, in turn, is divided into two groups: primary (if the infection initially penetrated only into the spinal cord) and secondary (if inflammation occurred after infection penetrated the spinal cord from other foci).
The people were taken aback! Joints will recover in 3 days! Attach...
Few people know, but this is exactly what heals joints in 7 days!
The causes of infectious myelitis most often include: herpes simplex virus types I and II, cytomegalovirus infection, mycoplasmas, syphilis, HIV, enterovirus infections. Somewhat less frequently, the etiological factor may be meningococcal infection and borellosis.
Secondary infectious myelitis occurs mainly with osteomyelitis of the spine and when infection is carried through the blood.
Traumatic, intoxication and other types of myelitis
. Intoxication myelitis occurs under the influence of poisons that are tropic to the cells of the spinal cord. Such inflammation can occur both during acute poisoning (for example, with a number of drugs and psychotropic drugs) and during chronic exposure to a toxic substance (most often this concerns hazardous production).
In addition, spinal inflammation can be caused by certain systemic diseases. Most often, myelitis can be found against the background of multiple sclerosis (in this case, myelitis can rightfully be called a symptom of the underlying disease), a number of autoimmune diseases and vasculitis.
Myelitis also often develops as a component of paraneoplastic syndrome, which occurs in the early stages of malignant tumor growth.
A precipitating factor - be it an infection or injury - causes swelling of the spinal cord. This can be considered the starting point from which the entire pathological process begins. Edema disrupts blood circulation in the tissues, and vascular blood clots occur. This in turn increases swelling.
A circulatory disorder (or even its cessation in certain areas) ultimately causes softening and necrosis of the spinal cord tissue.
After recovery, the site of necrosis is filled with connective tissue - a scar is formed.
Of course, scar tissue cannot perform the functions inherent in nerve cells, so many disorders that occur during illness can persist after recovery.
The clinical picture of myelitis depends entirely on the location of the inflammation. The level of damage is determined by segments or sections of the spinal cord (each of which has several segments).
For example, myelitis can be thoracic, upper cervical, lumbar, etc. As a rule, myelitis covers the entire diameter of the spinal cord segment, disrupting the functioning of all conduction systems.
This means that both spheres are disrupted: motor and sensitive.
It is worth describing the symptoms of myelitis taking into account the time of their onset. From the onset of the disease to its peak, the clinical manifestations of the disease change markedly. The first signs of infectious myelitis are completely nonspecific and differ little from other infectious diseases.
An acute onset, a sharp increase in body temperature to 38-39˚C, chills, weakness - all “standard” signs of any inflammatory process. Then the disease begins to acquire its characteristic features. The first neurological symptom is usually back pain. It can be very intense (this varies from person to person).
Pain in myelitis is not localized in one area: the pain spreads to neighboring areas of the body. Its irradiation (actually, the spread of pain) is a sign of damage to the roots of the spinal cord (radiculitis). The pain can “radiate” to the back, perineum, hips, etc. It all depends on the level of the lesion.
Symptoms become more severe over time, and in some cases this “evolution of symptoms” can occur over a period of hours or days.
As already mentioned, the clinical picture of myelitis varies depending on the level of inflammation. Myelitis of the upper segments of the cervical spinal cord is characterized by spastic tetraparesis. It is the most dangerous: there is always a possibility of damage to the phrenic nerve. This, in turn, threatens to stop breathing.
The spread of inflammation from the upper cervical segments upward to the structures of the medulla oblongata can lead to bulbar disorders. Myelitis at the level of the cervical thickening is manifested by a combination of flaccid paresis of the arms with spastic paresis of the legs. The lower segments of the cervical spine are affected more often than the upper ones, and their inflammation is not as dangerous.
In some cases, it threatens with persistent motor impairments (myelitis of this localization, as a rule, is not life-threatening).
The response to testing the knee and Achilles reflexes in thoracic myelitis is always too active.
It is worth remembering that with rapidly developing transverse myelitis, decreased muscle tone may first be observed, then, after some time, the disorders acquire the character of spastic paralysis.
The lumbosacral spinal cord is also often affected by myelitis. Symptoms of myelitis of this localization include peripheral paresis in the legs and disorder of pelvic functions such as urinary and fecal incontinence. In parallel with this, the muscles that are innervated by the affected nerves, deprived of normal regulation and nutrition, gradually atrophy.
Sensory disturbances are observed in any type of myelitis. The only unshakable rule: this kind of disorder always occurs below the site of the lesion.
Sensitive disorders consist of a decrease or complete absence of pain sensitivity, a decreased reaction to touch, cold, etc.
Paresthesia may occur - “non-existent sensations”, for example, “pins and needles”, cold or the feeling of wind.
There are no non-traumatic methods for diagnosing myelitis (of course, if you need to establish the exact cause and not a preliminary diagnosis). The most complete information is provided by a lumbar puncture. In acute cases, CT or MRI of the spine and myelography are prescribed.
Liquor puncture also makes it possible to carry out differential diagnosis, that is, to clarify the diagnosis by comparing the data obtained with the signs of clinically similar diseases.
Myelitis must be differentiated from Guillain-Barré syndrome, hematomyelia, epiduritis, tumors and acute circulatory disorders of the spinal cord.
When choosing treatment, a neurologist must rely on information about the possible cause of the disease and the characteristics of the development of myelitis in a given patient.
If necessary (based on the patient’s condition), muscle relaxants and uroseptics can be prescribed. For urinary retention, anticholinesterase drugs, bladder catheterization and rinsing with antiseptics are used.
Of great importance in the treatment of myelitis and its consequences is physical therapy (during bed rest - in bed, and later - in the hall or ward), massage (percussion) and physiotherapy. To restore the function of damaged nerve cells (as far as possible), it is necessary to use vitamin preparations (group B).
It is desirable that these are injectables. In order to prevent bedsores, various devices (cotton swabs, a circle) are placed under the sacrum and other bony protrusions, the position of the body is changed, and the skin is wiped with camphor alcohol or a soap-alcohol solution.
For the same purpose, UV irradiation is prescribed for the sacro-gluteal and ankle areas.
The prognosis for myelitis, again, depends on the level and extent of the lesion. Upper cervical myelitis often causes death in patients; lumbar and thoracic (without timely treatment) are highly likely to lead to disability.
With a favorable course of the disease, recovery occurs in 2-3 months, and full recovery occurs in 1-2 years.
During this period, it is recommended: sanatorium-resort treatment (if it is prescribed correctly, the duration of recovery will be significantly reduced), vitamin therapy, prevention of bedsores, physiotherapeutic procedures (UVR), physical therapy, and the prescription of anticholinesterase drugs.
Source: https://www.krasotaimedicina.ru/diseases/zabolevanija_neurology/myelitis
Treatment program
Treatment of myelitis in the acute and subacute stages of the process is carried out in a neurological hospital.
Drug treatment
The following drugs are used in the treatment of myelitis:
Drugs for treatment
Non-drug treatment and folk remedies
In the chronic stage of the process, the following are used to eliminate residual neurological symptoms:
The myostimulation procedure is the main component of physiotherapeutic treatment
Acupuncture is an effective method of rehabilitation for spinal cord myelitis
Folk remedies have not proven their effectiveness, so they are not used for spinal cord myelitis.
Diet
For myelitis, it is necessary to consume foods rich in vitamin B:
Prognosis and complications
The prognosis for treatment of spinal cord myelitis largely depends on the cause of the disease and the location of the inflammatory process. With inflammation in the cervical and thoracic spinal cord, the prognosis is serious due to damage to the respiratory muscles. With the inflammatory process of other localizations, lifelong persistence of varying degrees of severity of neurological symptoms is inevitable. The mortality rate for this disease reaches 30%.
Complications of the disease:
Stories of patients who survived spinal cord myelitis.
I have infectious transverse myelitis.
Got sick at 16 years old. Now I'm 50. I'm living. The disease is rare. Mostly happens at a young age - 14–20 years. Pilgrim
Myelitis can be post-infectious and post-traumatic.
I have post-infectious. The majority have post-traumatic. There are already four of us here who have unsubscribed. Post-infection probably manifested itself differently for everyone. It has all sorts of types and subspecies. And the level of damage may vary. But mental trauma from the fact of disability with any myelitis. Marquise https://www.disability.ru/forum/index.php?id=10467
Myelitis does manifest itself in different ways.
I met two “colleagues” in misfortune. The symptomatology of the consequences of myelitis in all three (including me) is lower spastic paraplegia. This is the main problem. Spasticity complicates a lot of things and we haven’t yet learned how to fight it effectively, except with a surgeon’s knife. Medication methods lead to a bunch of additional problems and complications. Well, besides doctors, there is also the person himself and his desire to live. Pilgrim https://www.disability.ru/forum/index.php?id=10467
Prevention
Preventive measures include:
Vaccine prevention is the main method of preventing spinal cord myelitis
Spinal cord myelitis is a serious neurological disease that is fraught with the development of dangerous complications. Timely diagnosis and treatment of the pathological process are vital for a favorable prognosis. Carrying out all necessary measures for vaccine prevention of infectious diseases is the main way to avoid the development of an inflammatory process in the spinal cord, associated complications and subsequent disability.
I have a higher medical education and work experience
Transverse myelitis is an inflammatory disease that affects the myelin sheath of the spinal cord (SC).
Subsequently, the bodies and processes of nerve cells, spinal cord roots, as well as blood and lymphatic vessels are involved in the pathological process.
The disease occurs with equal frequency in men and women; the age groups at risk are people from 10 to 19 and from 30 to 39 years, of which 28% of cases are children.
Depending on the location of the inflammatory process:
- focal - there is one focus of the disease in the spinal cord;
- multifocal - more than one focus of inflammation;
- transverse - is focal, but a distinctive feature is that the inflammation covers several adjacent spinal segments;
- diffuse - the lesion is distributed throughout the spinal cord, and is expressed to varying degrees.
By duration:
- spicy;
- subacute;
- chronic.
The definition of “transverse” does not mean that the entire diameter of the SM is involved in the process. This part of the term reflects the manifestation of a violation of surface sensitivity with the formation of a clear transverse level.
Vascular diseases of the brain
The brain (cerebrum)
is an organ of the central nervous system, consisting of many interconnected nerve cells and their processes.
Vascular diseases of the brain are recognized in medicine as one of the most dangerous groups of diseases, as they have quite serious consequences for the body. Each cerebral vascular disease has characteristic features that depend on which specific vessels are affected by the pathological process. But in any case, doctors at OKB No. 1 warn that diseases in this group can provoke a hemorrhagic or ischemic stroke, after which the patient either becomes disabled or dies.
Clinical manifestations of vascular diseases of the brain can be divided into the following forms:
- chronic cerebral ischemia stage I-II;
- cerebral circulatory disorder of a transient nature;
- cerebral infarction (ischemic stroke);
- bleeding in the brain (hemorrhagic stroke).
Causes of cerebrovascular diseases:
The occurrence of cerebrovascular diseases occurs as follows: insufficient blood supply limits the access of oxygen and glucose, resulting in a cerebral infarction, the results of which are unpredictable. In adulthood, vascular atherosclerosis and hypertension can negatively affect blood supply.
Treatment of vascular diseases of the brain:
Among the many diseases of the cerebral vessels, coronary disease and discirculatory encephalopathy deserve special attention.
Treatment of ischemic disease involves:
- work on restoring impaired physiological and behavioral functions, for which restorative therapy, magnetic and electrophoresis, physical therapy, and massage are used;
- stabilization of blood pressure and prevention of strokes with the help of anticoagulant and vasodilator drugs;
- normalization of metabolism and proper blood circulation. The best results are ensured by taking medications according to medical prescriptions.
Vegetative vascular dystonia
Vegetative-vascular dystonia is a disturbance in the functioning of the body’s vascular system, leading to insufficient oxygen supply to tissues and organs. Otherwise, this disease is called neurocirculatory dystonia, or cardiac neurosis.
Causes of VSD:
- Exhaustion of the body due to acute or chronic infectious diseases or intoxications.
- Sleep disturbances such as insomnia, early awakening or difficulty falling asleep.
- Chronic fatigue, depressed mood, depression.
- Irregular unbalanced diet.
- Excessive physical activity or physical inactivity.
- Hormonal changes in the body during puberty in adolescents, pregnancy or menopause in women.
- Change of climate or time zone.
Types of vegetative vascular dystonia:
With a more accurate diagnosis, three types of vegetative-vascular dystonia are distinguished:
- if, with general signs of fatigue, you sometimes have a feeling of lack of air, you complain of irregular heartbeats, then this is vegetative-vascular dystonia of the cardiac type;
- The hypotensive form of vegetative vascular dystonia is characterized by low blood pressure, general weakness, headaches, coldness of the fingers and toes, and a tendency to faint;
- periodic surges in blood pressure indicate hypertensive vegetative-vascular dystonia.
Diagnosis of VSD:
The diagnosis of vegetative-vascular dystonia is made only after a comprehensive examination of the patient and the exclusion of other pathologies that have similar manifestations to VSD.
The list of diagnostic measures includes:
- Laboratory research of general blood test, biochemical composition of plasma, coagulation indicators, hormone levels. If necessary, urine tests are performed. Most often, the indicators of these studies do not go beyond normal values.
- Functional techniques, including ultrasound examination of internal organs and blood vessels of the head and neck, ECG, monitoring of blood pressure levels.
- X-ray of the spinal column, tomography of the brain and spinal cord.
- Consultations with specialists in related specialties.
Only after confirming the absence of other diseases can a diagnosis of vegetative-vascular dystonia be made.
Treatment of vegetative-vascular dystonia:
The majority of patients with VSD do not require drug therapy. The basis of treatment for them is methods aimed at changing the patient’s lifestyle and normalizing the functioning of the nervous system. Physiotherapeutic methods are mainly used to treat the disease. This could be hydromassage, physical therapy. If the symptoms of vegetative-vascular dystonia are serious, acupuncture, manual therapy, and herbal medicine give good results. Vegetative-vascular dystonia responds well to treatment. The main thing is not to self-medicate. The choice of methods by which to treat vegetative vascular dystonia should be determined only by a doctor after conducting the necessary research. Often, VSD “masks” another disease, so its treatment should be aimed primarily at eliminating the underlying disease. And, of course, first of all, don’t bring yourself to the point of needing to see a doctor: try to avoid stressful situations and emotional breakdowns, and, if possible, take a few days of rest and spend them as you would like for a long time. Thus, treatment of vegetative vascular dystonia should be based on both drug therapy and regulation of the mental state.
Causes
Etiological classification of transverse myelitis:
- Infectious.
It is the cause in 50% of pathology cases:
Infectious transverse myelitis should be divided into two types: primary (the infection initially affected the SM) and secondary (the infection entered the SM from other foci by hematogenous route)
- Postinfectious myelitis.
Develops approximately 4 weeks after diseases such as measles, whooping cough, chicken pox, etc.; - Traumatic.
Occurs as a result of spinal injury, which can lead to damage to the spinal column and infection to the existing wound; - Intoxicating.
Occurs due to damage to SM cells by poisons as a result of poisoning. Among such poisons may be medicinal and narcotic substances, heavy metals (such as mercury, lead), etc.; - Vaccine-associated myelitis.
Develops after oral administration of a live vaccine containing a weakened polio virus; - Radiation myelitis.
Develops as a result of damage to the brain by ionizing radiation.
It is worth noting the advantage of an inactivated vaccine, which is not capable of causing disease, because contains killed polio virus.
Routes of infection
Ways of infection with infectious transverse myelitis:
- Fecal-oral. For example, if the disease is caused by the polio virus;
- Airborne (poliomyelitis virus, influenza virus);
- Transmissible, i.e. through insect bites (tick-borne encephalitis virus);
- Hematogenous. As mentioned above, a secondary focus in the SM can form when the infection spreads from primary foci (for example, with tuberculosis);
- Infectious agents can enter the spinal cord through open spinal trauma;
- Through animal bites (rabies virus).
Symptoms
Increase in general temperature to 39-40°C, general weakness. Pain localized at the site of the affected area of the spinal cord.
The cervical and thoracic regions of the spinal cord are most often affected, and less commonly the lumbar region.
Pain localized along the midline of the body in the dermatome corresponding to the affected area of the spinal cord (dermatome is a segment of skin innervated by one spinal cord root).
Neurological disorders are based on the destruction of the myelin sheath, which disrupts the efferent (descending, centrifugal) and afferent (centripetal, ascending) transmission of impulses in the nervous system. Symptoms associated with this pathological mechanism begin 2-3 days after the onset of the disease.
Neurological disorders:
- Pelvic disorders – disturbance of urination and defecation (possible development of ascending cystitis followed by sepsis). Observed when the thoracic segments of the SM are affected.
- Paraparesis manifests itself in the weakness of certain muscle groups of both limbs (lower or upper): monoparesis - decreased muscle strength in one limb; triparesis – in three limbs; hemiparesis – in the limbs of one half of the body; tetraparesis – muscle weakness in all four limbs. Appears when the upper segments of the cervical spine are affected.
- Breathing disturbance, even to the point of stopping. It develops in cases where the lesion affects the phrenic nerve.
- Reduced motor activity or its complete absence (paralysis) in the lower extremities, urinary and fecal incontinence - with damage to the lumbar segments of the spinal cord.
- Sensory disturbances below the site of the pathological focus.
- A change in gait that occurs due to paresis of the lower extremities (the patient drags his leg while walking).
- Reflexes: Babinsky - when the handle of the hammer is lightly passed along the lateral edge of the foot, in response to irritation the patient extends the toes in a fan-shaped manner; Oppenheim - when the handle of the hammer is passed along the crest of the tibia, pathological extension of the big toe of the tested leg is observed; Schaeffer - when the Achilles tendon is compressed, the big toe extends; Gordon - when the calf muscles are compressed, there is a slow extension of the big toe, and a fan-shaped divergence of the remaining toes of the same foot.
Some people experience cramps in their toes. Let's look at why this happens and what to do.
Signs of diseases and types
Signs of spinal cord disease are varied. Conventionally, this organ is divided into segments associated with a specific pair of spinal nerves. Each pair is responsible for a specific area of the body. It is worth noting that the nerve fibers of the gray matter intersect, so pathological processes on the left are manifested by dysfunction of the right side.
Movement disorders
Restriction of movement can be complete (paralysis) or partial (paresis). These symptoms are combined with either increased or decreased muscle tone. If the pathology affects all limbs - this is tetraparesis, two upper or two lower ones - paraparesis, one - monoparesis, the left or right half of the body - hemiparesis. As a rule, motor disturbances are symmetrical, but there are exceptions if the lesion is localized or the pathology is located in the area of the cauda equina (sacrum).
Injuries in the area of the 4th cervical vertebra are very dangerous. Pathology located above it causes disruption of the diaphragm, which leads to rapid death. Pathology below the vertebra leads to breathing problems, which can end tragically if help is not provided in time.
Sensory disorders
Symptoms, nature and location of disorders depend on the location of the pathology and its degree.
Damage to the peripheral parts of the spinal cord leads to a decrease in superficial and skin sensitivity, as well as temperature, pain and vibration. Paresthesia (tingling, numbness) is common.
Autonomic disorders
They are manifested by changes in body temperature, sweating, metabolic disorders, changes in the nature of stool, urination, defects in the functioning of the digestive system, etc.
Painful sensations
When the spinal cord is compressed, pain appears in the middle of the back; pinched cervical nerves lead to pain in the arms; Pathology of the lumbar region is reflected by pain syndrome of the lower extremities. All symptoms of spinal cord disease depend both on the affected substance (white or gray) and on the location of the damage. There are 5 segments: cervical, thoracic, lumbar, sacral and coccygeal.
Root damage
Almost all fibers of the spinal cord roots, which are responsible for motor, sensory and autonomic functions, are almost always affected. Isolated lesions are very rare. Pathology manifests itself as follows:
- pain in the innervation zone (area of influence of nerve fibers);
- numbness or tingling;
- paresthesia;
- paresis in the innervation zone (sometimes manifested by the appearance of a forced position);
- changes in the tone of innervated muscles;
- muscle tremors;
- feeling of cold or heat, impaired sweating.
Damage to several roots, unfortunately, is not excluded. This is polyradiculoneuritis. The listed symptoms get worse.
Pathology of the anterior horns of the gray matter is manifested by paralysis, atrophy of muscle tissue, twitching in the affected segment, pathology of the posterior horns - a decrease in several types of sensitivity in the affected area; lateral horns - a manifestation of Horner's syndrome (it is associated with vision and eye structures), if the defect is located at the level of the 5th cervical - 1st thoracic vertebrae.
Peripheral nerve damage
Many nerves are mixed and perform all the basic functions, so their disorders affect movements, sensitivity and autonomic functions. All this is accompanied by pain, paresis or paralysis.
Thoracic defect:
- leg paralysis;
- loss of sensitivity in the area below the ribs;
- disruption of internal organs;
- if the pathology is located in the upper thoracic region - respiratory failure;
- if there is a defect in the 3-5 thoracic vertebrae, there is a disruption of the heart.
This pathology is characterized by paralysis and complete loss of all types of sensation in the legs and perineum, radicular pain, and severe lower back pain.
Sacral lesion
This form of the disease greatly affects the quality of life. It is characterized by:
- severe pain in the legs, perineum and sacral area;
- loss of sensitivity of the above zones;
- paresis or paralysis of leg muscles;
- reduction of all reflexes in this area;
- disruption of the internal organs of the pelvis (impotence, bowel and bladder incontinence, etc.).
Damage to the coccyx is accompanied by:
- pain in this area and in the lower abdomen;
- inability to sit;
- increased pain when walking.
Diagnosis and treatment
The diagnosis of transverse myelitis is made on the basis of symptoms, in which neurological disorders play an important role.
A comparative description of symmetrical limbs is carried out, tests for pathological reflexes, and a study of muscle strength, which is assessed on a special scale.
The patient is asked to perform the movement characteristic of the joint and, counteracting with the hand, the muscle strength is determined:
- 5 – the patient offers good resistance to the doctor’s force;
- 4 – the force is minimally reduced, the patient resists the doctor’s actions, but is forced to use more force;
- 3 – the strength is reduced more than in the previous version, the doctor manages to prevent the limb from bending;
- 2 – the patient’s movements are possible only in a relaxed position or with the help of a doctor;
- 1 – the patient does not move, but the doctor feels the tension of his muscles;
- 0 – no movement, no muscle tone.
MRI and CT diagnostics are used to detect the location and extent of spinal cord damage.
In a general blood test, leukocytosis is observed with a shift to the left (i.e., blast forms of leukocytes predominate), increased ESR (erythrocyte sedimentation rate), increased fibrinogen and C-reactive protein, and antibodies to infectious agents.
The composition of the cerebrospinal fluid may not change, but sometimes increased protein, autoantibodies, and increased lymphocytes are detected.
Treatment
Conservative treatment:
- antibacterial drugs;
- antiviral drugs;
- analgesics;
- sedatives;
- antipyretics;
- strict bed rest;
- glucocorticosteroids.
To prevent urinary retention, anticholinesterase drugs are used; if they do not help, then catheterization of the bladder is performed.
Prevention of bedsores:
- soft cushions are placed under the sacral area and under the heels;
- the skin is wiped with a weak solution of manganese or camphor alcohol;
- physiotherapy.
To improve the conduction of nerve impulses, vitamin B is prescribed. After treatment, sanatorium-resort treatment and physical therapy are recommended.
Surgical treatment is indicated in the presence of purulent foci in the vicinity of the spinal cord and when compression of the spinal cord occurs.
The danger of transverse myelitis lies in the damage to such a highly organized structure as nervous tissue. Its destruction, followed by scar formation, leads to lifelong complications in motor activity and sensitivity of body parts, in particular the upper and lower extremities.
The disease is not self-curable and requires emergency medical care in a hospital setting, so preventing irreversible complications is only possible if you immediately contact a medical facility.
Basic principles of treatment of viral infections of the spinal cord
All treatment procedures are carried out in a hospital. The main method of treatment is drug therapy in the form of a course of antibiotics and sulfonamides, in addition, the patient is given an intravenous solution of hexamethylenetetramine and glucose.
To prevent bedsores, it is very important to carefully monitor your skin from the first days of illness. If bedsores do appear, then quartz irradiation and ointment dressings are necessary. Urinary retention is treated with a catheter in the bladder.
For viral infections of the spinal cord, prevention of contractures, passive and active gymnastics, and massage are also necessary.
Video on the topic
Subscribe to our Telegram channel @zdorovievnorme
Myelitis is an inflammatory disease that affects the spinal cord. The immune system begins to actively produce antibodies under the influence of certain damaging factors. They bind to foreign agents so that active cells of the human immune system have the opportunity to destroy them.
Because of such a struggle, the leukocytes themselves begin to die. Certain substances are released that penetrate the body's tissues and begin to destroy its cells. As a result, damage occurs to the gray and white matter of the spinal cord.
This condition is extremely dangerous, as it can cause irreparable harm to health, as well as lead to the progression of dangerous complications. This disease affects people from different age categories. The disease has no restrictions regarding gender.
Structure of the spinal cord
The spinal cord is part of the central nervous system. It supplies data and impulses to the brain. The main job of the spinal cord is to adequately transport the orders of the brain to the internal organs and muscles. It contains a variety of nervous tissue that signals from the brain to the body and back.
The spinal cord consists of white and gray tissue, nerves and the cells themselves. In the middle of the spinal cord, in the many nerves, there is pure nerve tissue.
If pathologies or traumatic effects involve the spinal region, this can result in a great danger to normal functioning and the quality of a person’s life. In addition, there is a risk of death. Even small compressions caused, for example, by spina bifida, can reduce sensitivity and mobility and negatively affect the functioning of internal organs. There are a huge number of symptoms of such disorders, but one thing remains unchanged - damage and disease in the area of the spinal canal are noticeable immediately.
Classification
In medicine, clinicians use several classifications of myelitis, which are based on the mechanism of development of the pathology, prevalence, reasons for the progression of the pathological process, as well as the duration of the disease.
By duration:
- acute myelitis.
The onset of the disease is violent. The symptoms are very pronounced. This disease is the most severe and many complications can develop against its background; - subacute type.
Symptoms begin to appear gradually. But it is worth noting that the nature of this pathology is progressive. This suggests that gradually the clinical picture will only worsen; - chronic type.
As a rule, the disease affects older people, but it can also develop in young people due to autoimmune disorders.
By prevalence:
- limited.
Only one pathological focus is localized in the spinal cord; - diffuse.
Inflammation covers the entire spinal cord; - multifocal.
In certain areas of the organ there are several foci (more than two); - transverse myelitis.
The development of this form is said to occur if the inflammatory process simultaneously affects several segments located next to each other.
According to the development mechanism:
- primary myelitis.
The disease develops independently (under the influence of unfavorable factors); - secondary myelitis.
The reason for the progression of this type of pathology is background diseases that are already developing in the human body. As a rule, these are processes with a chronic course.
Due to development:
- radial;
- bacterial;
- post-vaccination;
- viral;
- traumatic;
- idiopathic;
- toxic.
Pathologies and their clinical signs
Common symptoms when disorders occur include dizziness, nausea and muscle pain. Depending on the specific pathology, symptoms may be variable and of moderate severity. Common symptoms of spinal cord disease are:
- loss of sensation,
- severe pain in the spine,
- fecal and urinary incontinence,
- paralysis of the lower and upper limbs,
- psychosomatic symptoms,
- atrophy of muscle tissue.
Patients become limited in movement and complain of severe pain in the muscles and joints. The clinical picture depends on which substance is affected by the pathological processes. It is impossible to miss the manifestations of changes.
Spinal cord compression disease
Patients exhibit a whole range of neurological signs. They occur due to displacement and deformation of the spinal cord. Compression sickness disrupts its functioning. Its source is pathological formations or displacement of the vertebrae.
Such diseases include epidural abscess. It can affect any part of the spine. The pathology provokes infectious processes in the brain and spinal cord.
Occurs after otitis media, inflammation of the paranasal sinuses. The same thing happens against the background of bone osteomyelitis. Without adequate treatment, serious complications appear in the form of meningitis and meningoencephalitis.
Why is spinal puncture dangerous?
Find out how to treat spinal cord myelitis.
The group of compression diseases includes hematomyelia (bleeding into the spinal cord). An accompanying symptom is acute transverse myelopathy with severe pain. Pathological processes develop after injury or against the background of damage to the spinal vessels.
Symptoms of the disease appear depending on where it is located. This may be the cervical spinal cord, the thoracic segment, or the lumbar region. It is necessary to undergo a medical examination and treatment prescribed by a doctor.
Brain tumors
When pathological formations develop, it is important for doctors to determine their location. Considering the origin and location, spinal cord tumors are divided into several types:
- Extradural neoplasms. Malignant tumors that are characterized by rapid growth. They have a destructive effect on the spinal cord.
- Intradural. Extramedullary tumors, which form in most cases under the dura mater.
- Intramedullary. Pathological tumors that contain glial tissue. Their main location is the substance of the spinal cord.
To diagnose diseases, doctors prescribe neurological tests, x-rays, magnetic resonance imaging (MRI) and computed tomography (CT) to patients. In most cases, patients are recommended to undergo surgery. The results from using medications are short-lived.
Non-compression neoplastic myelopathies
Intramedullary metastases, as well as radiation and paracarcinomatous myelopathy, are more often diagnosed. There are no signs of external compression; CT and MRI results will show swelling of the spinal cord. Radiation therapy is used for treatment.
Progressive necrotizing myelopathy belongs to a non-compressive group of spinal cord diseases. Pathological processes affect neighboring segments and provoke mild inflammatory processes.
More often, progressive necrotizing myelopathy occurs after serious cancerous tumors. Patients experience spastic paraparesis, which leads to disturbances in the functioning of the pelvic organs.
How to treat tethered spinal cord syndrome?
Carcinomatous meningitis of the spinal cord. Pathological processes disrupt the functioning of the central nervous system. Blood pressure rises, epileptic seizures appear, brain function is disrupted, and the patient feels constant drowsiness.
Myelopathy and inflammation
In most cases, doctors diagnose arachnoiditis in patients (photos of patients). The disease refers to inflammatory pathologies that affect the brain or spinal cord.
Specialists prescribe an additional detailed examination to establish an accurate diagnosis. The inflammatory process is a consequence of previous otitis, sinusitis, or develops against the background of intoxication of the human body.
Acute myelitis also manifests itself with characteristic symptoms after the development of a viral infection. The patient requires emergency qualified assistance. It is important to promptly identify the source of infection. The disease is characterized by paresis and weakness in the body, which quickly increases.
Infectious myelopathy occurs after herpes zoster. The pathology is complex and requires qualified treatment over a long period. The clinical picture is pronounced, it is difficult for the patient to understand and correctly describe his condition.
Vascular diseases
The source of pathological processes are congenital anomalies, changes in the walls of blood vessels or compression lesions. In rare cases, vascular diseases of the brain and spinal cord develop against the background of an abnormal structure of the capillaries themselves.
Pathological changes can occur in the human body without characteristic signs over a long period.
Common signs of vascular diseases of the spinal cord are the following manifestations:
- headache,
- weakness in the body,
- sleep disturbance,
- dizziness,
- loss of consciousness,
- high blood pressure,
- irritability,
- problems with memory and attention,
- impaired coordination of movements.
Therapy is prescribed by a doctor based on the results obtained after a thorough examination and diagnosis. Incorrect treatment can worsen the patient’s condition, and pathological processes will begin to actively progress. In some situations, surgery is required to restore blood circulation to the spinal cord.
How to treat spinal cord cancer?
Find out what to do if you have a spinal cord stroke.
Heart attack and its consequences
Changes in spinal circulation lead to serious disturbances in the functioning of the spinal cord. The flow of blood becomes difficult, causing a heart attack. Any part of the spine is at risk.
More often, pathological processes develop in areas of severe damage. The cause is difficult to determine, but in most cases it is a blood clot in small blood vessels. They carry blood to the spinal cord even when the extravertebral arteries are damaged.
Spinal cord infarction is most often diagnosed in people over 50 years of age. It is provoked by a blood clot or dissection of the aorta, damage to the main vessel of the spinal cord (traumatic disease).
The causes of the disease can also be arteritis and serum pathology. Against the background of spinal circulation disorders or myelischemia, a general ischemic infarction develops. Pathological processes affect several parts of the spinal cord at once.
The clinical picture in each case is varied. Patients complain of severe pain in the back. Temperature and pain sensitivity decreases.
In some situations, bilateral mild paralysis of the upper and lower extremities appears. A severe spinal infarction is indicated by constant pain in the head, nausea and weakness, accompanied by loss of consciousness.
The consequences of ischemic myelopathy include paresis of one or more limbs, while muscle weakness remains. The acts of defecation and urination are disrupted, and it is difficult for a person to control these processes. There are areas on the body where sensitivity is reduced or completely absent. Rarely does a heart attack lead to the death of the patient.
Chronic illness
Osteochondrosis is a dangerous disease, after which serious complications arise. In most cases, pathological processes cannot be reversed. The reason is that 95% of patients avoid a preventive visit to a specialist.
The disease cannot be detected at an early stage of development. A person goes to the hospital when he is no longer able to tolerate specific signs of pathology.
At a late stage, osteochondrosis provokes the development of spondylosis. The disease develops against the background of dystrophic changes in the tissues of the spinal cord. Bone growths (osteophytes) compress the spinal canal and cause problems.
Under the influence of strong pressure, stenosis of the central canal occurs. A dangerous disease that triggers pathological processes that spread to the brain and central nervous system.
Treatment of spinal cord disease is symptomatic in most cases. Doctors select effective therapy to alleviate the patient’s condition. The most positive result is considered to be stable remission, when specialists manage to delay the progression of pathological processes. Most spinal cord diseases cannot be reversed.
Degeneration and heredity
Hereditary degenerative pathologies are accompanied by a variety of clinical signs, but the course of the diseases is similar. The first symptoms in a person occur after the negative influence of the provoking factor on the central nervous system.
Gradually the patient's condition worsens, pathological processes progress.
Hereditary degenerative diseases of the spinal cord negatively affect the functions of the human body. We are talking about hearing, vision, thought processes. The same goes for speech and movement. In most cases, the cause of the development of pathology is a gene.
Etiology
Many unfavorable factors can provoke the progression of myelitis:
- traumatic myelitis.
In this case, the cause of myelitis progression is injuries to the spinal column, due to which viral or bacterial agents can penetrate the spinal cord; - viral.
Infection of the body with viruses, and; - post-vaccination.
They begin to develop in people who have recently been vaccinated and are prone to developing allergic reactions; - bacterial.
Often this type of spinal cord lesion begins to develop against the background. The infectious agent is meningococcus. Less commonly – tuberculosis bacillus or treponema pallidum; - toxic.
The disease progresses after poisoning the body with certain toxic substances. Most often, alcohols and salts of heavy metals act as poisons; - autoimmune.
The development of pathology is observed due to the fact that the body begins to independently produce antibodies against its own cells.
Factors in the development of the disease
The main causes of myelitis are caused by:
- lesions of the spinal cord (poliomyelitis, etc.);
- injury to the spinal column;
- various types of intoxications (salts of heavy metals, alcohols, organic solvents, etc.);
- demyelinating diseases that are caused by the breakdown of the nerve fiber sheath (multiple sclerosis, etc.);
- weakening of the immune system and general hypothermia.
When it is impossible to establish the cause of the disease, the pathological process is classified as idiopathic, but it is assumed that the main factor in such symptoms is provoked by a malfunction in the immune system.
Symptoms
Regardless of what caused the inflammatory process in the spinal cord, the clinical picture of different types of myelitis is similar:
- intoxication syndrome.
It is expressed very clearly. A person’s temperature rises, appetite decreases, nausea and vomiting are observed; - cerebral symptoms.
Such symptoms occur due to increased intracranial and spinal pressure. The victim has a headache with uncontrollable vomiting, which has no connection with food intake. It tends to intensify under the influence of certain stimuli, such as loud sounds or bright lights.
Focal symptoms directly depend on the stage of development of the inflammatory process in the spinal cord. It is worth noting here that the main physiological function of the spinal cord is to conduct nerve impulses from the brain to certain tissues and organs in the body. If an inflammatory process develops in one of the segments, then the entire chain is disrupted, and the following symptoms occur:
- impairment of motor activity. In this case, both a mild form (paresis) and complete immobility of a person (paralysis) can be observed;
- sensitivity disorder. The severity of symptoms directly depends on the size of the inflammatory focus. Sensitivity can either decrease (until complete anesthesia) or increase. In some cases, paresthesia is observed - sensations may be distorted.
Arachnoiditis of the meninges (cerebral)[edit | edit code]
Cerebral arachnoiditis can be localized on the convex surface of the brain, its base, in the postcranial fossa. The clinical picture of arachnoiditis consists of symptoms of local effects of meningeal lesions on the brain and liquor circulation disorders. A common manifestation of cerebral arachnoiditis is headaches of a hypertensive or meningeal nature.
The normal circulation of cerebrospinal fluid (CSF) through the cerebral ventricles is complicated by arachnoiditis of the meninges and may be disrupted.
Arachnoiditis of the convexital surface of the brain is more common in the anterior parts of the cerebral hemispheres, in the area of the central gyri. Due to pressure on the motor and sensory centers, movement disorders (mono- or hemiparesis) and sensitivity may occur. Irritation, and in cases of cyst formation, compression of the cortex and underlying parts of the brain during arachnoiditis cause focal epileptic seizures.
In severe cases, generalized convulsive seizures may occur, leading to the development of status epilepticus. Electroencephalography and pneumography are important for identifying the localization of the focus of arachnoiditis.
Diagnostics
If you notice the first symptoms that indicate the possible development of myelitis, you must contact a medical facility as soon as possible to diagnose the disease. An accurate diagnosis is made after a medical specialist examines the patient, as well as after laboratory and instrumental examination techniques.
Laboratory methods:
- immunological tests;
- bacteriological tests;
- cerebrospinal fluid analysis.
Instrumental methods:
- ENMG.
Treatment
Treatment of myelitis should begin as soon as the diagnosis has been confirmed. In this case, the chances of its success increase several times. Doctors use both drug and non-drug treatment methods.
Drug treatment:
- the first thing to do. This is to eliminate the cause of the disease. For this purpose, doctors prescribe the patient to take antiviral drugs and antibiotics;
- eliminate inflammation. GCS and immunosuppressants are prescribed;
- symptomatic therapy. To eliminate unpleasant symptoms, painkillers, diuretics, etc. are prescribed;
- prevention of complications.
Non-drug therapy is used during the recovery period. Physiotherapy, exercise therapy, and aquatherapy have a good effect.