Hypertension syndrome
Increased intracranial pressure occurs as a result of an increase in brain volume and disruption of hemo- and liquor dynamics.
Compression of the cerebrospinal fluid pathways and the appearance of excessive amounts of fluid in the intercellular spaces lead to the development of cerebral edema, an important role in the pathogenesis of which belongs to hemodynamic disorders and mechanical disturbances of blood circulation. An increase in venous pressure in the choroid plexus promotes hypersecretion of cerebrospinal fluid and a decrease in its resorption. An increase in intracranial pressure leads to a decrease in cerebral blood flow, the development of hypoxia of nervous tissue, and disruption of cerebral metabolism.
Cerebral edema, hypoxemia and ischemia cause severe metabolic disorders in nervous tissue and death of nerve cells. A feature of the development of cerebral edema in children is its diffuseness and rapid spread due to insufficient development of the blood-brain barrier and increased hydrophilicity of the brain substance.
The degree of increase in intracranial pressure depends on the location of the tumor and its size. Small tumors located in the confined space of the posterior cranial fossa can cause pronounced cerebral symptoms, as they quickly disrupt cerebrospinal fluid dynamics and cause an increase in venous pressure due to compression of the venous sinuses. Hemispheric tumors located far from the cerebrospinal fluid pathways and venous channels can be asymptomatic for a long time.
Symptoms of intracranial hypertension are headache, vomiting, dizziness, mental disorders, epileptic seizures, congestive optic discs, and radiological changes in craniograms.
Hypertension headache has a very typical clinical picture - it is diffuse, bursting in nature with some predominance in the frontotemporal, occipito-cervical regions, often occurs in the morning or in the early morning hours, and then goes away after some time. At first, it is episodic, but as the tumor progresses, the headache increases and becomes permanent, with periodic exacerbations—hypertensive crises.
Local headaches are not typical for brain tumors, but can occur from irritation by a growing tumor (most often a meningioma) of the sensory endings of the cranial nerves involved in the innervation of the dura mater with its falciform process and cerebellar tentorium.
Vomiting most often occurs in the morning on an empty stomach at the height of a headache without preliminary nausea and does not depend on meals. In children, it may be the first symptom of a tumor of the posterior cranial fossa, in particular the fourth ventricle. This vomiting should be differentiated from vomiting at the height of dizziness with Meniere's syndrome, with migraine and a number of other diseases, and in children with helminthic infestation.
With dizziness, patients experience lightheadedness, darkening of the eyes, loss of balance, and unsteadiness or uncertainty when standing and walking. Dizziness can be accompanied by a number of autonomic reactions - nausea, vomiting, paleness of the skin, tinnitus and even fainting. This symptom also occurs in other diseases, in particular in circulatory failure in the vertebrobasilar system.
Mental changes are observed very often and are characterized by memory and orientation disorders, changes in the patient’s personality, character, and behavior. In addition, patients have weakened attention, there is mental retardation, stupor and darkening of consciousness.
Epileptic syndrome occurs on average in 30.2% of cases and depends on the localization of the process. It can be either a local sign or a hypertensive one.
Intracranial hypertension causes a decrease in blood pressure, especially diastolic pressure, bradycardia, and circulatory disorders. Cardiovascular disorders are a consequence of the direct influence of high cerebrospinal fluid pressure on the regulatory centers of the brain stem.
Congestive optic discs in patients with brain tumors (BTT)
occur in 70-78% of cases and are a very valuable objective symptom of venous stagnation and increased intracranial pressure.
Complicated congestive optic discs. In 1953, E. J. Tron identified a special clinical form of congestive discs, in which, along with an increase in intracranial pressure, the main pathological process itself affects the visual pathway. With prolonged stagnant discs, secondary atrophy of the optic nerves may occur.
Foster Kennedy syndrome is expressed in the development of simple atrophy on the side of the lesion, decreased vision up to complete blindness, and a congestive disc on the opposite side.
Craniographic signs of intracranial hypertension are characterized by the following changes - osteoporosis of the dorsum of the sella turcica, widening of the entrance to it and deepening of the bottom of the sella turcica. Occasionally, increased vascular patterns and digital impressions are noted on the bones of the skull.
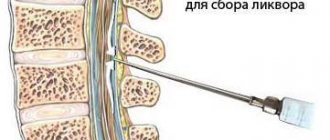
In addition to the listed main signs of increased intracranial pressure, meningeal symptoms, protein-cell dissociation of the cerebrospinal fluid, respiratory and pulse disturbances, and changes in the electroencephalogram may be observed.
As an example, we can cite tumors of the pineal region, which most often manifest themselves with hypertension syndrome - headaches, nausea, vomiting, ataxia, congestive optic discs. In this case, the leading symptoms are paresis of upward gaze (Parinaud's symptom), Argyll-Robertson's symptom. More rare signs are diplopia, diabetes insipidus, changes in visual fields, abducens nerve paresis and a number of others. With magnetic resonance imaging, these tumors are visualized quite well, and concomitant occlusive hydrocephalus is often detected.
Classic won't help?
For many years it was believed that you can raise a harmonious person if you play classical music for him from childhood. Various musical compositions written by Mozart , Bach, Chopin and other eminent masters were supposed to develop the brain. In reality, everything turned out to be wrong. Already in 1993, a study was conducted at the University of California at Irvine, which showed that listening to Mozart can improve spatial thinking in a person, but... exclusively and for no more than 15 minutes. Moreover, this result is also subject to doubt, since scientists have not been able to obtain a similar result in any other study or experiment.
Another study on this topic was structured like this: one group was given to listen to Mozart, the other was given to read Stephen King . And the results after reading the books were similar to the results after listening to the maestro. So the researchers concluded that a person’s spatial imagination improves when they are in a good mood, either caused by listening to music or reading a book.
Focal neurological symptoms
Tumors of the cerebral hemispheres are clinically divided according to the signs of damage to the corresponding lobes of the brain.
The frontal lobe occupies a significant part of the cerebral hemisphere, extending anterior to the Rolandic fissure, and at the base reaching the pituitary infundibulum and the Sylvian fossa. However, in clinical practice, the frontal lobe is understood as the anterior part of the hemisphere, lying anterior to the prepentral sulcus. Posterior to the postcentral gyrus is the parietal lobe, which is divided into superior and inferior, then the occipital and temporal lobes are distinguished, the latter is also divided into the anterior third, middle and posterior.
Tumors of the frontal lobes are characterized by the following symptoms:
1) epileptic seizures of various types; 2) peculiar disorders of higher nervous activity, known as the “frontal” psyche; 3) impaired coordination of movements in the form of frontal ataxia (disorders of standing and walking); 4) isolated disturbance of innervation of the facial muscles according to the central type; 5) impaired sense of smell; 6) peculiar dysfunctions of the optic nerves with basal localization of the pathological focus.
Other, more rare symptoms are also observed: grasping reflexes and oral automatism, motor aphasia, impairment of counting, writing, and reading. It should be noted that damage to the right frontal lobe may not produce clear symptoms of loss or irritation of functions.
Seizures of general epilepsy occur much more often with glioblastomas than with meningiomas. In this case, a general epileptic seizure that appears suddenly “like thunder on a clear day” should alert the clinician and refer the patient for a comprehensive neurosurgical examination. In some cases, with glioblastomas, epileptic seizures turn into an epileptic state - “status epilepticus”.
With meningiomas, general epileptic seizures are observed less frequently than focal ones; neurological symptoms with meningiomas are closely related to their location.
With tumors of the frontal localization, the state of higher nervous activity is often disturbed - patients are inhibited, stunned, and insufficiently active, although consciousness and orientation are preserved. Stunning syndrome is observed more often with rapidly growing metastatic tumors, with glioblastomas; with meningiomas it occurs less frequently and occurs later. “Frontal” psychopathological syndrome is characterized by a loss of the ability to restrain one’s desires, emotions, and statements; patients lose the upbringing skills that make a person acceptable in society and sociable.
Against the background of general stupor, apathy, and passivity, patients often display excessive “swaggering,” talkativeness, a tendency to shallow jokes, and cynicism; some become hypersexual; many of them are unclean, their urination behavior is disrupted, and this does not bother them; Despite the obvious severity of the condition, patients remain euphoric.
Olfactory impairment occurs in 1/3 of patients and occurs not only with basally located tumors, but also with others located far from the primary olfactory elements. With unilateral tumors, not only unilateral, but also bilateral smell disturbances can be observed. Stagnant optic discs are more common in glioblastomas than in patients with benign gliomas and metastases. They occur comparatively less frequently with meningiomas.
In case of acute processes in the frontal lobe (hemorrhage into the tumor), symptoms of damage to the area of voluntary rotation of the eyes and head appear - deviation of the eyeballs towards the lesion. When this area is irritated, convulsive twitching of the eyes and head occurs in the opposite hemisphere.
Tumors of the central gyrus or Rolandic region are characterized by early impairment of motor or sensory functions, depending on the starting point of development of the tumor: in the area of the anterior central gyrus or the posterior gyrus, or both. When irritated, typical cortical Jacksonian epilepsy is noted. A seizure begins from a specific, strictly limited group of muscles on one side.
As the tumor destroys the motor cells of the cortex, epileptic seizures gradually disappear, giving way to paralysis. Sometimes the disease begins with the development of mono- or hemiparesis, plegia. Tumors of the posterior central gyrus exhibit the same symptoms. Irritation phenomena cause attacks of paresthesia in the form of tingling sensations, numbness, dull pain, burning, etc. Subsequently, the muscular-articular sense, stereognostic sense, and, to a lesser extent, tactile and temperature sensitivity are impaired.
Tumors of the superior parietal lobe
With damage to the superior parietal lobe, especially on the left, astereognosis and apraxia are observed.
With astereognosis, the patient, feeling an object taken in the hand opposite to the lesion, can feel and describe its individual properties, but cannot create an image of the object - cannot recognize it. With apraxia, the patient loses the ability to perform complex goal-directed actions. Damage to the right superior parietal lobe is accompanied by autopagnosia, pseudopolymyelia, pseudoalelia, and anosognosia. When the inferior parietal lobe is damaged on the left, the so-called Gerstmann syndrome is determined - acalculia, alexia, agraphia, finger agnosia, sensory aphasia.
Tumors of the occipital lobe are rare and cause visual impairment in the form of quadrant or half hemianopia, visual agnosia, metamorphopsia, micropsia, and visual hallucinations.
If the temporal lobe of the right hemisphere is affected, there may be no focal symptoms, and therefore signs of increased intracranial pressure appear early. The headache is often bilateral. Congestive optic discs may be detected before focal symptoms occur. The most typical symptom of a tumor is epileptiform seizures. They can be large or small, often in the form of absence seizures. The seizure is often preceded by an olfactory or gustatory aura. There may be auditory and visual hallucinations.
When the Graciole bundle is involved in the pathological process, patients first develop quadrant, and then the same hemianopsia of opposite visual fields. Tumors of the left temporal lobe may cause sensory aphasia due to damage to Wernicke's area. Patients lose the ability to understand speech.
Unlike patients with motor aphasia, patients with damage to the posterior parts of the temporal lobe are excessively talkative and even talkative, but speech becomes incorrect - letters are replaced or words are placed incorrectly. Speech becomes “foreign”. Amnestic aphasia is also observed - the ability to determine the “name of objects” is lost.
Focal symptoms of cerebellar tumors are often bilateral in nature, since in children to whom they are characteristic, the tumors are often localized in the vermis. Nystagmus, coordination disorder, decreased muscle tone are observed, static coordination is impaired; the patient cannot stand, sit, and falls in the Romberg position. When the lower parts of the cerebellar vermis are involved in the pathological process, the patient deviates backward; when the upper parts are affected, the patient deviates forward. Gait disturbance is typical: the child staggers in both directions and often falls. Static ataxia is combined with asynergia.
Damage to the hemispheres is characterized by scanned, unevenly modulated speech, nystagmus is often horizontal, large-scale. On the side of the tumor, symptoms of damage to the V, VI, VII, VIII nerves may be observed: decreased corneal reflex, strabismus, diplopia, asymmetry of the nasolabial folds, dizziness and tinnitus, as well as ataxia in the limbs on the affected side (overshooting, dysmetria, hypermetria, adiadochokinesis and muscle atony). During the process in the upper parts of the hemisphere, it is mainly the arm that suffers, and in the lower parts the leg. When walking, the patient deviates towards the affected hemisphere.
Depending on the histological variant of the cerebellar tumor, the dynamics of the disease changes. With benign tumors - astrocytomas - symptoms increase slowly, focal ones can appear 1-2 years after the onset of the tumor; cerebral symptoms during this time are unstable, remissions are possible. In the case of medulloblastoma, the increase in symptoms is very rapid - within several months, characterized by general physical exhaustion and the appearance of additional focal symptoms indicating supratentorial or spinal spread of the process.
One of the common symptoms of a cerebellar tumor is a forced position of the head with an inclination in the direction opposite to the lesion of the cerebellar hemisphere, less often in the same direction. When an attack of headache occurs, the position changes, it is thrown back or brought forward to the chest.
Gliomas are the most common tumors of the brain stem. Initially, one of the cranial nerves is affected. Then an alternating syndrome develops. As the tumor grows, symptoms become bilateral; boulevard or pseudobulbar syndrome, paresis and paralysis of the limbs occur. Tumors growing from the outer surface of the trunk first manifest themselves as symptoms of damage to the cranial nerves, then conduction disorders occur.
When the tumor is localized in the midbrain, oculomotor disorders, ptosis, diplopia, convergence disorder, accommodation disorder, strabismus, and often alternating Weber syndrome develop. Damage to the roof of the midbrain is accompanied by paresis of upward or downward gaze, vertical, converging nystagmus, hearing loss, and ataxia. Hypertensive symptoms appear later.
When a tumor of the bridge occurs, paresis of gaze towards the lesion, alternating syndromes of Millard-Gubler, Foville, ataxia, and autonomic disorders occur. When the tumor is localized in the medulla oblongata, breathing and cardiovascular disorders, bulbar and pseudobulbar palsies, and alternating Jackson and Schmidt syndromes develop.
With tumors in the area of the fourth ventricle, liquorodynamic disturbances and attacks of occlusion are observed, characterized by the appearance of a sudden headache, vomiting, sometimes a disorder of consciousness, difficulty breathing and cardiac activity (Bruns syndrome). Tumors of the cerebellopontine angle (neurinoma of the VIII nerve) cause a sensation of ringing in the ear and dizziness. Then symptoms of damage to the facial, trigeminal and abducens nerves appear, and cerebellar disorders appear.
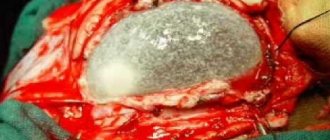
As an example of how tumors of the same histological structure (meningiomas, neuromas of rare localization) manifest themselves depending on their location, let us consider the clinical symptoms of these OGMs.
With convexital location of meningiomas, symptoms of irritation from the parts of the brain that are subject to the tumor predominate, which are subsequently replaced by symptoms of prolapse, as well as the development of intracranial hypertension syndrome. With basal localization, symptoms of damage to the cranial nerves come first, along with the development of a slowly increasing syndrome of intracranial hypertension.
With meningiomas of the olfactory fossa, the symptoms of the disease are hypertensive headaches, decreased vision due to secondary atrophy of the optic nerves, and damage to the olfactory nerves. Meningiomas of the main bone site are characterized by the presence in patients of general seizures, simple atrophy of the optic nerves, and headaches of a meningeal nature.
With meningiomas of the tubercle of the sella turcica, the first symptom of the disease is a significant unilateral decrease in vision due to the development of simple atrophy of the optic nerve, followed by loss of visual fields and decreased vision on the other side. The development of meningiomas of the wings of the sphenoid bone causes symptoms of irritation of the temporal lobe, which is manifested by seizures, olfactory or visual hallucinations. The rapid development of intracranial hypertension syndrome is also characteristic.
Meningiomas of the posterior cranial fossa are characterized by the development of intracranial hypertension syndrome along with damage to the nerves of the lateral cistern of the bridge (V, VI, VII, IX cranial nerves). It should be remembered that meningiomas can have intraosseous and intraventricular localization. In rare cases, these tumors manifest as intracranial hemorrhages.
As for multiple meningiomas, the situation here is somewhat different and the clinical symptoms, while remaining dependent on the location, are also determined by other factors. D. A. Gulyaev identified 3 variants of their clinical course.
The first option is characterized by a long-term asymptomatic course of the disease in the structure of neurofibromatosis type 2, the clinical manifestations of which manifest themselves first and complicate the diagnostic process. A certain dependence of the course of the disease on the nature of the phenotypic manifestations of neurofibromatosis has been revealed. The more pronounced the phenotypic signs of neurofibromatosis, the higher the likelihood of patients with multiple intracranial meningiomas. This may be due to multiple mutations both in the neurofibromatosis type 2 gene itself and, possibly, in other genes.
The second option is characterized by the clinical manifestation in patients with primary multiple intracranial meningiomas without phenotypic manifestations of neurofibromatosis. Due to the slow, non-invasive growth of the tumor and gradual compression of the underlying medulla, the patients went to a medical institution for general cerebral symptoms.
The third variant of the clinical course belongs to the group of sequentially multiple intracranial meningiomas. In these observations, focal neurological symptoms come to the fore. The period from the first manifestations of the disease to seeking specialized medical help is shorter than in patients with neurofibromatosis type 2 or primary multiple intracranial meningiomas.
Neuroma of the VII nerve is manifested by a slow loss of its function, although sometimes symptoms can occur acutely, simulating acute neuritis. In half of the cases, symptoms of damage to the facial nerve are accompanied by noise in the ear and dizziness. In some cases, palpation in the area of the mastoid process under the ear reveals a dense tumor mass, and sometimes otorrhea is observed.
Schwannomas of the jugular foramen develop rarely and are manifested by various syndromes involving the IX, X, XI nerves:
Wernet's syndrome - damage to the IX, X, XI nerves; Collet-Sicard syndrome - involvement of the IX, X, XI and XII nerves; Villaret's syndrome - involvement of the IX, X, XI, XII cranial nerves and superior sympathetic ganglion.
Features of functional brain asymmetry
Each person is individual, differing in character, temperament, specific memory and thinking, manners and skills from another person.
Undoubtedly, the educational process and society leave a serious mark, but the main reason is considered to be the functioning of the central nervous system.
Functional asymmetry of the brain determines the characteristics of the hemispheres regarding emotional manifestations and high mental activity.
Features of asymmetry
Functional asymmetry of the brain is characterized by the placement of mental functions relative to the right and left hemisphere. It has been proven that the activity of the left hemisphere consists of handling significant information, reading and counting.
The work of the right one consists of operating with images, orientation on the ground, distinguishing sounds in music; recognition of objects, people's appearance; as well as reproducing dreams.
The hemispheres work interconnectedly, representing their individuality on the functionality of the brain.
Its formation occurs in close connection with society during the public development of the individual. The hemisphere, which is responsible for the functioning of the speech apparatus, should be considered dominant. Most people, according to this theory, have a dominant left hemisphere and are considered right-handed. Left-handers, on the contrary, have a mirror image in the action of their thinking.
Based on the dominant hemispheres, all people are divided into 3 categories:
- Left-hemisphere - make up 42% of the total number.
- Right-hemisphere - 10 - 20% of the population.
- Equihemispheric - have equal formation of the two hemispheres of the brain, accounting for 40%.
Left-handed (right-hemisphere) people have always generated interest among the public because of their individuality. Previously, such people were feared, bringing unflattering meaning into this. At the same time, there is no disease to be left-handed. Psychological disorders are not observed in people; they are considered an individual trait of a person.
According to statistics, left-handers often become writers, journalists, artists, and organizers. But among right-handers, engineers, mathematicians, philosophers, and linguists often appear.
The simplest method to determine the principle of brain asymmetry is to compare the formation of the left and right upper limbs.
People who write with their right hand are right-handed and, of course, left-brained. For left-handed people the opposite is true.
There are a small number of people who have the ability to use both limbs with equal dexterity. This feature is called ambidexterity with congenital and acquired manifestations.
Each person’s definition of hemisphere dominance and the principles for placing specific functions among them are quite individual.
The division of functional responsibilities between the hemispheres is genetic. At the same time, due to the influence of social reasons, a change in the functional asymmetry of the brain occurs.
The function of the hemispheres for relatively simple work (sensory organs, skeletal muscles) is considered by scientists as conditionally equipotential. The symmetry sections of the hemispheres equally contribute to movement and a certain perceptibility.
Interhemispheric asymmetry occurs:
- anatomical – manifested in the morphological confusion of hemispheres;
- biochemical – expressed in differences in cell reactions and the presence of neurotransmitters;
- psychological – motor, sensory, cognitive-emotional.
The functional asymmetry between the hemispheres determines the responsibility of the left hemisphere for the result of verbal information, and the right hemisphere for changes in visual and figurative patterns.
Separation of functional loads
Each of the hemispheres has its own tendency to work, producing a unique and unique combination of personality during a common action. The advantage in brain performance of one hemisphere leads to an increase in personal characteristics in one direction.
People with right hemisphere asymmetry are characterized by contemplation, subtle sensitivity, and a disposition to rush into the jungle of memories.
A person with predominant functioning of the right hemisphere often exhibits slowness and taciturnity. Left-hemisphere people are characterized by analytical thinking and iron logic.
Theoretical knowledge comes easily to them, they have a developed vocabulary, they are active and purposeful.
The main signs of the left hemisphere:
- logical and important analytical abilities of the brain;
- consideration of abstract form;
- the ability to assimilate events, dates, names;
- speech function with testing of oral dialect and ability to learn foreign languages;
- the ability to determine similarity among objects;
- the ability to perform difficult motor acts;
- the ability to remember past moments according to an abstract, generalized and invariant type;
- the ability to evaluate time relationships;
- the ability to identify similarities by names.
The signs of the right hemisphere are as follows:
- consideration by type of specificity;
- musical gift;
- the ability to notice the emotional tone and affiliation of another person’s speech;
- the ability to correctly assess the nature of non-speech sounds;
- the ability to perceive a specific visual object;
- the ability to recognize certain incidents;
- simultaneous holistic and general perception;
- the ability to evaluate spatial relationships;
- the ability to establish distinctive features among objects;
- the ability to indicate similarities with respect to physical stimuli;
- assumptions, dreams.
Both hemispheres are interconnected in their influence, providing a person with a holistic range of qualities. However, each of them adds its own share of uniqueness.
At the stage of formation of the first year of life, the right hemisphere dominates over the left hemisphere relative to its work. In the 2nd year of life, the left hemisphere catches up with it.
When some time passes, there is an alternation of superiorities over each other in formation.
The hemispheres are united by calloused flesh, which serves as a crossing between them and reaches residual formation at the age of 25. For females it is large.
The judgment of symmetry does not exist in the human body. The asymmetry of the hemispheres is closely related to the symmetry of the face. The human face is asymmetrical, which is considered normal. There is a noticeable connection between the face and the asymmetry of the hemisphere.
Often in right-handed people the nose is deviated to the right side, while in left-handed people it is deviated to the left side. If one eyebrow is raised, this is characteristic of a narrow part of the facial area, and a crooked smile indicates a wider area of the face.
Functional asymmetry of the cerebral hemispheres contributes to the harmonious functioning of cerebral systems, most often due to reciprocal relationships. In this case, it is possible to locate the functional pressure between 2 hemispheres, combine information and monitor 1 of the hemispheres.
Asymmetrical connection with floors
There is a close contact of asymmetry with the floor. Among stutterers, left-handed people, cross-eyed people, neurotics and children with dyslexia, there are 5 boys for every 1 girl.
It has been proven that there is a clear connection between these manifestations, and all of them are directly related to brain asymmetry.
For example, if a left-handed child is forcibly retrained to write with his right hand, he will often develop the following deviations, and they will also become mentally retarded, develop psychosis, and speech disorders.
Understanding of gender differences and brain functions was initially built on the results of clinical and behavioral experiments. If the left hemisphere is damaged due to blood loss, malignancy, or surgical intervention of the temporal lobe element in relation to epileptic seizures, lack of verbal performance in males occurs frequently.
Such violations of the right hemisphere also lead to a strong lack of non-verbal flow in men relative to women. The disease due to damage to the left hemisphere occurs in men 3 times more often with a severe course. Hence, the conclusion was presented that women's linguistic and spatial skills are represented more symmetrically compared to the male gender.
Psychological dimorphism is associated with gender differences in brain lateralization:
- Different skills and dispositions between the sexes.
- Diverse professional suitability, preference.
- Uneven learning ability, resourcefulness.
For example, regarding verbal skills (speech apparatus, speed of speech, spelling, short memorization, comfort of thought in all classes) - a high indicator for the female gender. They have a well-developed sense of smell, which does not atrophy over the years.
The male gender has a well-developed visual ability. In school, they understand geometric concepts more than girls. Also, men achieve much more success in chess, music, and creativity. There are few women who become satirists, humorists, and comedians.
Due to asymmetry, the brain constitution operates in a coordinated manner. Due to the fact that some of the brain's activities are divided regarding 2 hemispheres, the clinical course of a violation of one of the hemispheres will differ.
This makes it possible to identify functional asymmetry as an effective position in order to identify a large number of neurological ailments.
Only the single function of the 2 hemispheres, their asymmetrical work, will guarantee human life and activity.
Source: https://glmozg.ru/stroenie/osobennosti-funktsionalnoj-asimmetrii-mozga.html
Occlusive hydrocephalus
The closed form of hydrocephalus, depending on the level of obstruction of the cerebrospinal fluid tract, occurs with occlusion of the foramina of Monroe, aqueduct of Sylvius, IV ventricle, foramen of Magendie or Luschka, which is mainly caused by tumors.
In this case, the expansion of the ventricles occurs anterior to the site of blockage of the liquor system. OMG in both adults and children, especially with pathology of the posterior cranial fossa, with medulloblastomas, astrocytomas, ependymomas, cause varying degrees of severity of liquor circulation disorders, which are accompanied by excessive accumulation of cerebrospinal fluid in the craniospinal system and increased intracranial pressure.
The causes of these disorders in case of space-occupying formations are complete or partial occlusion of the cerebrospinal fluid pathways, impaired resorption of cerebrospinal fluid, and in case of tumors of the lateral ventricles - hyperproduction of cerebrospinal fluid.
Thus, tumors of the posterior cranial fossa and the resulting hydrocephalus lead to the development of hypertension syndrome, which significantly aggravates the patient’s condition, and before removing the tumor, it is necessary to correct the cerebrospinal fluid circulation, which is achieved through cerebrospinal fluid shunting operations.
Frontal
These lobes have a frontal location, they occupy the forehead area. Let's figure out what the frontal lobe is responsible for. The frontal lobes of the brain are responsible for sending commands to all organs and systems. They can be figuratively called a “command post.” It would take a long time to list all their functions. These centers are responsible for all actions and provide the most important human qualities (initiative, independence, critical self-esteem, etc.).
It is the frontal lobes that control human behavior. This part of the brain sends commands that prevent a specific antisocial action from being performed. It is easy to notice how this area is affected in dementia patients. The internal limiter is turned off, and the person can tirelessly use obscene language, indulge in obscenities, etc.
The frontal lobes of the brain are also responsible for planning, organizing voluntary actions, and mastering the necessary skills. Thanks to them, those actions that seem very difficult at first become automatic over time. But when these areas are damaged, the person performs the actions as if anew each time, and automaticity is not developed. Such patients forget how to go to the store, how to cook, etc.
When the frontal lobes are damaged, perseveration can occur, in which patients literally become fixated on performing the same action. A person may repeat the same word, phrase, or constantly move objects around aimlessly.
The frontal lobes have a main, dominant, most often left, lobe. Thanks to her work, speech, attention, and abstract thinking are organized.
It is the frontal lobes that are responsible for maintaining the human body in an upright position. Patients with their lesions are distinguished by a hunched posture and a mincing gait.
Parietal
In order to understand the functions of the parietal lobes, it is important to understand that the dominant and non-dominant side will do different jobs.
The dominant parietal lobe of the brain helps to understand the structure of the whole through its parts, their structure, order. Thanks to her, we know how to put individual parts into a whole. The ability to read is very indicative of this. To read a word, you need to put the letters together, and you need to create a phrase from the words. Manipulations with numbers are also carried out.
The parietal lobe helps to link individual movements into a complete action. When this function is disrupted, apraxia is observed. Patients cannot perform basic actions, for example, they are not able to get dressed. This happens with Alzheimer's disease. A person simply forgets how to make the necessary movements.
The dominant area helps you feel your body, distinguish between the right and left sides, and relate parts and the whole. This regulation is involved in spatial orientation.
The non-dominant side (in right-handed people it is the right side) combines information that comes from the occipital lobes and allows you to perceive the world around you in three-dimensional mode. If the non-dominant parietal lobe is disrupted, visual agnosia may occur, in which a person is unable to recognize objects, landscapes, or even faces.
The parietal lobes are involved in the perception of pain, cold, and heat. Their functioning also ensures orientation in space.
Temporal
They are responsible for hearing, turning sounds into images. They provide speech perception and communication in general. The dominant temporal lobe of the brain allows you to fill the words you hear with meaning and select the necessary lexemes in order to express your thoughts. The non-dominant helps to recognize intonation and determine the expression of a human face.
The anterior and middle temporal regions are responsible for the sense of smell. If it is lost in old age, it may signal incipient Alzheimer's disease.
If both temporal lobes are affected, a person cannot assimilate visual images, becomes serene, and his sexuality goes through the roof.
Recovery
Speaking about recovery, it should be noted what functions the brain performs and those that may be impaired:
- vision and hearing, smell;
- movements;
- speech;
- the ability to process information of any kind, to read, write;
- understanding the meaning of words;
- memory , both visual and verbal;
- abstract thinking.
The more severe the degree of brain damage, the more various functions are impaired. The recovery process often takes a long time. In many ways, the possibility of recovery depends on how quickly the victim received medical care.
During the recovery process, the patient takes medications, visits a massage room, and undergoes physiotherapy. Classes with a psychologist and speech therapist are of no small importance.
Manual therapy and kinesiotherapy are used, during which the patient is forced to move correctly in order to restore body functions.
source
Treatment
Before doctors arrive, primary care must be provided to the patient. While waiting for a medical team, you can improve your condition somewhat by doing a few things:
- Place the person on a surface covered with pillows, with the head raised.
- When you are in the house, open the window.
- Remove all constrictive clothing, unbutton your shirt and belt.
- If a person feels the urge to vomit, gently tilt his head to the side. This is done in order to prevent vomit from entering the throat and respiratory organs.
Doctors in a hospital setting provide basic and specific therapy, which helps minimize damage to nerve cells. Basic therapy is used to preserve the functioning of the brain and cardiovascular system. Specific measures are aimed at restoring blood circulation and brain tissue. The greatest effect is achieved with the combined use of methods.
If treatment does not produce results or is not effective enough, therapeutic and preventive measures and rehabilitation courses are carried out aimed at restoring body functions.
The doctor prescribes the patient to take medications from the following groups:
- Thrombolytics are used in the first hours after a stroke to resolve blood clots.
- Anticoagulants.
- Medicines to lower blood pressure.
- Vasoactive drugs.
- Neuroprotectors.
All medications are selected in accordance with the clinical picture of the stroke.