General description of acoustic neuroma
Since the vestibular-cochlear nerve consists of two parts at once - both vestibular and auditory, the clinical manifestations of its tumor lesions are varied. In the vast majority of cases diagnosed with neuromas of similar localization, people turn to an otolaryngologist with complaints of a sharp decrease in hearing function.
As the tumor grows, compression of adjacent intracranial structures is observed, which also contributes to the worsening of neurological symptoms - damage to the facial or trigeminal nerve, glossopharyngeal or vagus nerve bundle.
Due to the fact that the formation of a pathological focus occurs after a mutation of Schwann cells, practicing oncologists refer to the pathology as acoustic schwannoma.
The predominant age for the appearance of such foci of atypia in people is 30–45 years, but not a single case of auditory neuroma has been recorded in children. The prevalence of the pathology is 12–15% of all cerebral tumor lesions.
What happens in the body with schwannoma?
Symptoms of acoustic neuroma greatly depend on the stage of the disease - the size of the tumor. They are also influenced by the location of the tumor. As the tumor grows, it grows deeper, displacing the normal position of blood vessels, nerve endings and other tissues. Due to compression, symptoms intensify and new signs appear. Clinical picture:
Gradually increasing ringing in the ears. Acoustic neuroma on one side is accompanied by constant ringing in 7 out of 10 cases. In this case, ringing can appear even at a stage when the size of the tumor does not exceed 1-2 mm.
Hearing impairment . One of the main signs of the disease, hearing loss occurs gradually, but occurs in 95% of cases of the disease. First, the patient ceases to distinguish high-pitched sounds, then the neuroma of the nerve captures medium and low frequencies. There are complaints that the patient will not be able to distinguish voices on the telephone.
Loss of coordination and dizziness . Similar symptoms accompany acoustic neuroma in approximately 60% of cases. These symptoms occur only if the tumor has already reached a size of 4 cm or has become larger. Vestibular signs develop because the vestibulocochlear nerve consists of an auditory and vestibular part. Because of this, a disorder occurs that is confused with signs of VSD.
Symptoms of compression of the trigeminal nerve . They develop if the acoustic neuroma begins to actively grow. However, the symptom occurs in only 15% of clinical cases. If the trigeminal nerve is affected, this indicates that the size of the tumor has become more than 2 cm.
Signs of changes: impaired sensitivity of the skin and facial muscles, toothache and unilateral painful sensations. In later stages, pronounced chewing atrophy is observed.
Symptoms of damage to the abducens and facial nerves . They occur if the tumor becomes larger than 4 cm. The patient suffers from loss of taste, salivation worsens, and sensitivity is impaired. Sometimes, in later stages, strabismus or double vision develops.
As the acoustic neuroma grows, other parts of the brain are involved: the brainstem and the cerebellum located within it. If this happens, the patient loses the ability to speak, breathing and swallowing function is impaired, and blood pressure increases. In some situations, confusion and acute mental disorders are noticeable.
Symptoms
The growth of a benign formation takes a long period of time. At the very beginning of the disease, the signs are blurred, and sometimes they are not paid attention to. Symptoms become distinct in the last stages of the disease, and in 80% of cases they are diagnosed at the same time.
The symptoms of acoustic neuroma are as follows:
- slow hearing loss - may be temporary (it appears and then disappears);
- headaches, problems with coordination;
- perhaps partial numbness of the facial part on the side where the tumor is localized;
- nausea, very rarely vomiting;
- twitching of the eye when the tumor grows and puts pressure on the nerve endings;
- the occurrence of tinnitus;
- toothache;
- in the last stages there are problems with vision and mental health.
In the initial stages, the disease can be mistaken for neuralgia, labyrinthitis, or otosclerosis.
To the described symptoms are added problems with the voice and loss of taste.
It is very important to diagnose the pathology in time and begin treatment, which will allow you to maintain health and avoid unnecessary complications.
Morphology of the disease
The neoplasm macroscopically looks like a dense round or irregularly shaped node. Its surface is lumpy and has a connective tissue capsule on the outside. Diffuse or local cavities filled with brownish liquid may be observed inside the tumor. Depending on the blood supply, the neuroma has a pale pink, bluish or brownish color on the cut.
Microscopic examination reveals that acoustic schwannoma consists of cells with rod-shaped nuclei. The cells form a palisade-like structure, separated by fibrous areas. As the neuroma grows, it becomes fibrotic and deposits of hemosiderin are formed.
Causes and development factors
Ear diseases are quite specific and can be caused by all sorts of reasons, however, neuroma is not one of the list of hearing diseases that lend themselves to a standard description.
Thus, there are unilateral and bilateral forms of the disease. Bilateral is much less common, and the main cause of its development is neurofibromatosis.
Neurofibromatosis is inherited. The presence of this disease in the body indicates the patient’s predisposition to the development of benign tumors, including bilateral acoustic neuroma.
The cause of unilateral neuroma is still not completely known; doctors can only guess what causes this disease. So, possible causes of the development of neuroma include:
- irradiation of the body;
- poisoning with toxic substances;
- traumatic brain injuries;
- diseases of the cardiac system;
- presence of infectious diseases;
- ear diseases (otitis media, labyrinthitis).
Causes and consequences
Acoustic neuroma is idiopathic in most cases. This complicates its treatment, since without a clearly established cause it is much more difficult to influence the problem and its consequences.
However, there are several factors that can increase the risk of developing a tumor. First of all, like almost any other tumor, neuroma can appear under the influence of radiation. Radiation has a general negative effect on the body and provokes the degeneration of cells, their pathological reproduction and other similar processes. Radiation can be obtained due to the characteristics of professional activity, a man-made disaster, or through contact with radioactive substances. Minor doses during a medical examination do not have a negative effect, but tend to accumulate in the body. Some treatments also pose radiological hazards but have no alternative.
The second factor is heredity. A disease such as neurofibromatosis type 2 causes genetic mutations and provokes the growth of schwannomas and other benign formations. Patients with this diagnosis lose their hearing by the age of 30-40, and most often the tumor develops on both sides.
In addition to hearing loss, complete or partial, acoustic neuroma has other consequences:
- hydrocephalus;
- degeneration into oncology is rare;
- disability due to effects on certain areas of the brain and the development of hearing loss;
- death due to brain damage.
The main complication in the development of a neoplasm, despite its benign nature, is that it affects the soft tissues of the inner ear and brain. When schwannoma extends beyond the internal auditory canal, it affects nearby neurovascular structures. This causes a person to lose some sensations and functions. The main difficulty is that even after eliminating the problem, not all areas can be completely restored. In addition, the processes of neighboring nerves can be damaged during surgery.
What is an acoustic neuroma?
Acoustic neuroma is a tumor that affects the auditory nerve and nearby nerve tissues and structures. Due to the location of the auditory nerve near the brain, neuroma is quite dangerous. The consequences of the disease may include deafness, other hearing, vision, swallowing disorders and facial nerve paresis.
The auditory nerve is divided into two parts: the cochlear branch, which transmits sound signals from the external environment to the brain, and the vestibular nerve, which is responsible for the sense of balance. The primary focus of acoustic neuroma is in the nervous tissue that is connected to the vestibular apparatus. This fact leads to the fact that the disease affects not only the hearing system, leading to hearing loss, but also to the fact that the patient has problems with orientation in space and imbalance, that is, with precisely those body functions for which the vestibular system is responsible. apparatus.
Among tumor diseases of the brain, acoustic neuroma accounts for just over 10% and usually occurs in middle-aged adults. There are no pediatric patients with this disease. According to statistics, only one person in 100,000 gets sick with acoustic neuroma every year.
Clinical picture
Due to the slow growth of the tumor, there is a gradual development of the symptomatic picture, which is preceded by an asymptomatic period. In 95% of cases, the first sign is a gradual or sudden deterioration in hearing. In 60% - the appearance of ringing and noise in the ears. If compression of the auditory nerve is unilateral, patients may not notice the development of hearing loss for a long time. In 2/3 of cases, patients also have vestibular disorders. They are characterized by:
- Dizziness;
- Instability;
- Nystagmus;
- Vestibular crises accompanied by nausea and vomiting.
In typical cases, the first symptom of neuroma is hearing loss or, less commonly, dizziness. Hearing loss may be the only symptom of the disease, especially in the initial stages. At first, these disorders usually manifest themselves as signs of hearing irritation on the side of the tumor: patients hear various noises and sounds. The onset of murmurs usually precedes the onset of other symptoms. The sensation of noise may stop. Patients sometimes do not notice hearing loss for a long time, especially in the absence of tinnitus.
Dizziness in patients with acoustic neuromas develops and increases gradually. In some cases, they are in the nature of vestibular crises, accompanied by nausea and vomiting. An objective examination reveals horizontal nystagmus, which is more pronounced when looking towards the tumor. The cochlear (carrying auditory impulses) and vestibular parts of the auditory nerve are usually affected simultaneously. In some cases, only one part of the nerve is affected.
The next symptom to occur is paresthesia and pain in half of the face on the side of the tumor. The pain is usually aching, dull; in the first period of the disease they may at times intensify and subside. They are the result of compression by a neuroma of the trigeminal nerve, which runs next to the auditory nerve. Less commonly, the pain is paroxysmal in nature and at first may be mistaken for trigeminal neuralgia or associated with dental diseases. As compression of the nerve by the growing tumor increases, trigeminal pain becomes constant. At the same time, pain may appear in the corresponding half of the back of the head. Despite compression of the trigeminal nerve by the tumor, persistent trigeminal pain is rare.
Depression of the corneal reflex, weakness and atrophy of the masticatory muscles are also associated with damage to the trigeminal nerve. At the same time or slightly later, peripheral paresis of the facial and abducens nerves appears on the side of the tumor. Early appearance of peripheral paresis of the facial nerve is observed with neuromas located in the internal auditory canal. The growing tumor encounters resistance from the bones of the ear canal, which leads to increased pressure on the facial nerve. Clinically, this is accompanied by the appearance of paresis, loss of taste in the anterior two-thirds of the tongue and salivary disorders.
Diplopia (double vision) due to damage to the abducens nerve is at first transient in nature and only later becomes persistent.
The further development of the clinical picture depends on the direction in which the tumor grows.
As the tumor grows upward and posteriorly, symptoms of cerebellar damage occur. With growth downward and posteriorly, symptoms of damage to the glossopharyngeal and vagus nerves are added (disorders of phonation, swallowing, inhibition of the pharyngeal reflex, as well as sensitivity in the posterior third of the tongue). In advanced cases, dysarthria, dysphagia, atrophy of the muscles of the corresponding half of the tongue, and paresis of the accessory nerve may appear.
Despite compression of the adjacent parts of the brain stem and pushing it to the opposite side, conduction motor and sensory disturbances are weakly expressed. Damage to the pyramidal system is expressed in increased reflexes and the appearance of pathological foot reflexes on the opposite side. Severe paresis is extremely rare.
Increased intracranial pressure is a late symptom of the disease. As a manifestation of intracranial hypertension, congestion of the optic nerves develops. Due to pressure on the chiasm or optic tracts of the dilated third ventricle, changes in visual fields occur (bitemporal or binasal hemianopsia, scotomas). With the appearance of increased intracranial pressure, the headache becomes general in nature, focusing mainly in the forehead and back of the head. It is accompanied by vomiting.
Neuroma detection methods
You can sign up for diagnostics of acoustic neuroma after detecting the first signs. However, in rare cases, patients themselves discover the prerequisites for the formation of a tumor. It all starts with a visit to a neurologist and subsequent procedures:
- audiogram – the patient’s hearing is checked, the most vulnerable areas;
- electronystagmography – assesses the condition of the nerve that is responsible for the functioning of the vestibular apparatus;
- Ultrasound, X-rays and tomography of various types - the condition of the brain and surrounding tissues is visualized.
The doctor collects a medical history, a description of symptoms, and the presence of diseases in close relatives. Be sure to carry out differential diagnosis, which helps to distinguish acoustic neuroma from other ear and neurological diseases.
Classification and stages of development of acoustic neuroma
All classifications and stages of acoustic neuroma take into account the size of the tumor and its position relative to the brain stem. The classifications of W. Koos and M. Samii are actively used in medical practice. They allow you to determine treatment tactics.
Stages of neuroma growth according to W. Koos:
- Stage I - tumor up to 10 mm, does not extend beyond the internal auditory canal;
- Stage II - tumor up to 20 mm, expands the internal auditory canal and extends into the cerebellopontine angle;
- Stage III - tumor up to 30 mm, reaches the brain stem, but does not compress it;
- Stage IV - the tumor is larger than 30 mm and compresses the brain stem.
Classification of acoustic neuroma according to M. Samii:
- T1 - tumor located in the internal auditory canal;
- T2 - tumor growing from the internal auditory canal;
- T3a - tumor filling the cistern of the cerebellopontine angle;
- T3b - tumor reaching the brain stem;
- T4a - tumor compressing the trunk;
- T4b is a tumor that grossly deforms the brain stem and the 4th ventricle.
We can also distinguish four stages of the clinical course of the disease :
- otiatric stage - noise or deafness in one ear;
- otoneurological stage - lesions of the trigeminal and facial nerves on the side of the tumor are added;
- hypertensive-hydrocephalic stage - at this stage of the disease the patient notices headaches, nausea and vomiting;
- bulbar stage - dysarthria, dysphagia, dysphonia are added.
Consequences of an auditory nerve tumor
If the neuroma was diagnosed at the first or second stage, the probability of getting rid of the pathology without complications is high. Conservative treatment or radiation stops tumor growth. The tumor does not reach a large size, which saves the patient from compression of the adjacent nerves.
In the case of surgery, the success of therapy depends on the competence of the specialist and recovery in the postoperative period. Rehabilitation, lasting from 5 to 7 days and carried out in a hospital setting, includes taking medications that support the body.
The complete recovery period after excision of a neuroma is about a year. The prognosis is positive in case of high-quality tumor removal. Relapses are observed when small areas of neoplasm are left. In the third stage of the disease, important functions are disrupted. The patient is diagnosed with hearing loss and paralysis of the facial muscles.
Acoustic neuroma is classified as a benign tumor. This tumor is dangerous due to its location in the inner ear. The growing schwannoma compresses the auditory, optic and facial nerves. As a result of such exposure, the health and life of the patient are at risk. It is important to diagnose neuroma at an early stage.
Additional facts
VIII pair of the cranial nerve - the vestibular-cochlear, or auditory, nerve consists of the vestibular and auditory parts. The first carries information from the vestibular receptors of the cochlea to the cerebral centers, the second - from the auditory ones. In the vast majority of cases, neuroma develops in the vestibular part of the vestibulocochlear nerve, and symptoms of damage to the auditory department are associated with its compression by the tumor. Near the vestibular-cochlear nerve pass: the trunk of the facial nerve, the trigeminal nerve, the abducens, glossopharyngeal and vagus nerves. As the neuroma grows, symptoms of compression of these nerves, as well as adjacent structures of the brain stem, may appear in the clinical picture. Acoustic neuroma originates from Schwann cells surrounding the axons of nerve fibers. In this regard, in practical neurology it is also known as vestibular (acoustic) schwannoma. The incidence of the tumor is approximately 1 case per 100 thousand people. At the same time, acoustic neuroma accounts for 12-13% of all cerebral tumors and approximately 1/3 of tumors of the posterior cranial fossa. It develops mainly at the age of 30-40 years. Not a single case of the disease has been reported in prepubescent children.
Features of the course of the disease
The disease is characterized by a slow decrease in hearing in one ear. Often, such patients do not seek medical help for a long time or are observed by an otolaryngologist with an erroneous diagnosis of “cochlear neuritis” and only in the later stages undergo a full examination.
In most cases, the clinical manifestations of the disease depend on the stage of the tumor process, the size of the tumor itself and its growth rate. Small neoplasms with a long development cycle are often asymptomatic and can be discovered by chance.
As the neuroma grows, local symptoms first appear (hearing loss, tinnitus), and then neurological signs. However, in atypical cases, the disease may bypass ear symptoms and immediately present with signs of compression of the cranial nerves. As a rule, neuroma causes a unilateral pathological process, but cases of bilateral lesions have also been described (for example, with neurofibromatosis).
Affected Populations
Acoustic neuromas affect women more often than men. Most cases of acoustic neuroma develop in people between 30 and 60 years of age. Although quite rare, they also occur in children. Vestibular schwannomas are estimated to affect approximately 1 in 100,000 people in the general population. Racial disparities have been reported, with blacks, Hispanics, and people of Asian descent having relatively fewer neuroma diagnoses than people with white skin.
About 2,500 new patients are diagnosed every year. The incidence has increased over the past few years, which some researchers attribute to the increased recognition of small tumors. However, many people with small acoustic neuromas may remain undiagnosed, making it difficult to determine its true incidence in the general population.
Symptoms of acoustic neuroma
The main symptom of acoustic neuroma at the initial stage of the disease is hearing loss on one side. Additionally, there is tinnitus, pain in the nasopharynx and throat. Stimulants and physiotherapy are used as therapy. If such symptoms are caused by diseases other than acoustic neuroma, then recovery usually occurs quickly. And in cases of neuroma, such treatment leads to a worsening of the patient’s condition.
Any tumor tends to compress surrounding tissues and organs; a similar process occurs when the auditory nerve is infected with neuroma. As the tumor grows, the pressure on the auditory nerve, namely on its cochlear part, will increase, and this becomes the cause of hearing loss. When the neuroma is large, the brain stem and its important centers are compressed, which creates a danger to life.
As a rule, the tumor grows very slowly in neuromas, and it may take several years for the tumor to grow to a size at which the clinical picture of the disease becomes noticeable. Symptoms of damage to the auditory nerve may not appear during this entire time. To do this, the size of the tumor must become noticeable.
However, it is worth noting that the clinical picture of an acoustic neuroma can be bright even with small tumor sizes; here everything depends on the location of the tumor lesion of the auditory nerve. That is, the symptoms will depend on the location and size of the neuroma, while on the side of the lesion of the auditory nerve the symptoms will be more noticeable.
Symptoms of acoustic neuroma usually develop in the following sequence:
- hearing impairment on the side of the tumor, the development of which can occur gradually or occur suddenly; this symptom is characteristic of 95% of patients, as well as tinnitus;
- frequent dizziness, impaired balance and coordination of movements, that is, the vestibular function of the brain and the vestibular nerve in particular, so it is no coincidence that this disease is also called vestibular schwannoma, these symptoms occur in 60% of patients;
- tingling and numbness are felt in the face, which is associated with damage to the facial nerve, since with a certain localization of the tumor it negatively affects the functions of the facial nerve;
- problems with vision, taste, etc.
More about neuroma
Neuroma is a tumor of the auditory nerve that develops from the so-called Schwann cells, which form the supporting tissues of the cranial and auditory nerve pathways. These cells got their name from the German physiologist Theodor Schwann, who discovered them. Acoustic neuromas also have other names: acoustic neuromas or vestibular schwannomas.
The tumor process of the auditory nerves primarily disrupts the basic essential functions of these nerve trunks, which consist in transmitting sound impulses to certain brain centers for subsequent processing, which provides us with the ability to hear. In addition, these nerve trunks are also responsible for the functioning of the vestibular apparatus - a special device that allows us to control the position of the body in space, for example, to stand confidently on our feet. By the way, neuroma often forms precisely on the vestibular segment of the auditory nerve.
Acoustic neuroma is a benign tumor, also called acoustic neuroma.
Neuromas are not very common - for every 10 tumors of the central nervous system there is one acoustic neuroma, and in women these tumors are registered more often than in male patients. Most often, this pathology affects people at the most active age - from 30 to 40 years old, but it practically does not occur in children.
Acoustic neuroma is a serious disease that requires timely diagnosis and treatment.
A few words about the causes of neuroma development
As for the possible reasons for the development of this pathology, unfortunately, today medicine cannot answer this question. Moreover, experts find it difficult to identify probable risk factors leading to the formation of neuroma. In some cases, the development of acoustic neuroma occurs against the background of neurofibromatosis, a disease of a genetic nature.
Neurofibromatosis is characterized by the formation of neurofibromas - benign neoplasms in various segments of the central nervous system (CNS), including the auditory nerve. So, if you have a family history of neurofibromatosis, you are likely to be at increased risk.
Neuroma that occurs against the background of neurofibromatosis usually develops on both sides.
Symptoms of the disease
As already mentioned, a tumor that has arisen on the auditory nerve, as it develops, increasingly inhibits its most important functions. It should be noted that this tumor grows slowly and over a long period - up to several years. All this time it may not reveal itself in any way. Then, as compression of the nerve trunk increases, a characteristic symptomatic picture begins to develop:
- a decrease in hearing level on the side where the tumor has formed, which can either increase gradually or occur quite abruptly;
- ringing and extraneous noise in the affected ear;
- loss of coordination, uncertainty in movements, dizziness;
- involuntary eye movements (nystagmus);
- pain or even paralysis (paresis) of the facial (trigeminal) nerve, starting with numbness and tingling on one side of the face.
Tinnitus and hearing loss can be considered the earliest symptoms of the development of acoustic neuroma.
Depending on the size of the tumor, doctors distinguish three stages of the disease:
- The tumor does not exceed 2-2.5 centimeters in diameter;
- Reaches the size of a walnut;
- It is the size of a chicken egg.
As a rule, symptoms increase in direct proportion to the increase in size (stage) of the tumor, however, in some cases, a small neuroma can be located in such a way that it will put pressure on the surrounding tissues, forming a characteristic symptomatic picture.
It should be remembered that a neuroma may not reveal itself for a long time.
Diagnostics
For the most accurate diagnosis of the disease today, specialists have the opportunity to use a whole arsenal of tools that allow them to choose the optimal method of treatment. The following methods are used to diagnose neuroma:
- computed tomography (CT) and magnetic resonance imaging (MRI);
- X-ray examination;
- Ultrasound;
- electronystagmography (recording of involuntary movements of the eyeballs);
- drawing up an audiogram measuring hearing level, conducting hearing tests;
- biopsy of tumor tissue.
Recent Entries
Is it possible to give a mirror: how to protect yourself from bad omens It became known about the influence of cell phone towers on human health Is it possible to eat bananas bought in Russia?
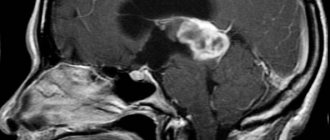
MRI is one of the ways to diagnose neuroma
Stages of neoplasm
Neuroma is divided into three stages:
- In the first degree, the pathology is small in size (up to 2.5 cm in diameter) leads to typical hearing impairment, as well as vestibular disorders. In addition, disruptions in the functionality of taste buds occur, and the facial nerve is slightly damaged.
- At the second stage, the size of the neoplasm resembles a walnut. Due to pressure on the brain stem, the patient suffers from impaired motor coordination, the formation of nystagmus, as well as dysfunction of balance and sudden movements of the eyeballs.
- At the third stage, the tumor already has the appearance of a chicken egg, as a result of which the cerebral structures are suddenly compressed, hydrocephalus develops, and vision and swallowing deteriorate.
During the last stage, brain tissue changes irreparably, and the neoplasm itself becomes inoperable, which ends in death.
Clinical stages
At the first stage of the disease, a person is concerned about hearing loss in the affected ear.
According to the size of the tumor, 3 main stages of the disease are distinguished. Let's take a closer look at them.
- In the initial stage of the disease, the tumor is small (up to 15 mm) and is located deep in the internal auditory canal. During this period, patients are concerned about hearing loss or deafness in one ear and noise in it. At the same time, taste disorders are observed in the anterior 2/3 of the tongue and vestibular disorders. The examination reveals hearing loss with clear lateralization of ultrasound in the healthy direction, relatively normal perception of pure tones and the inability to understand speech. In addition, such patients experience a decrease in the sensitivity of the cornea, nasal mucosa and oral cavity. Sometimes, in its debut, acoustic neuroma manifests itself with pronounced vestibular symptoms and can mimic Meniere's disease or labyrinthopathy.
- In the second stage, the size of the neuroma reaches 40 mm, it extends beyond the pyramid of the temporal bone and puts pressure on the brain structures (cerebellum, pons, medulla oblongata). Moreover, all clinical symptoms are clearly expressed. Other signs of the disease include nystagmus (involuntary movements of the eyeballs), static disorders (impaired coordination of movements, instability when walking), attacks of dizziness become more frequent and intensified, and the first signs of intracranial hypertension (papilledema) appear. The nuclei of the trigeminal nerve may also be affected, which is manifested by paresthesia in the area of its innervation and trismus of the masticatory muscles on the affected side.
- The tumor continues to grow and can be larger than 60 mm. Against the background of progressive neurological symptoms, ear symptoms fade into the background. In patients, intracranial hypertension increases, there is severe multiple nystagmus, and mental disorders develop. During this period, signs of damage to the cranial nerves (facial, vagus, trigeminal), and sometimes visual, are expressed, resulting in blindness.
As a result, the disease leads to damage to vital centers (respiratory and vasomotor) in the medulla oblongata and death.
It should be noted that, taking into account modern diagnostic capabilities and oncological alertness of health workers, the last stage of the disease is extremely rare.
Diagnostics. Neuroimaging of acoustic neuromas
Computed tomography (CT) and magnetic resonance imaging (MRI) are methods that, for acoustic neuromas, as well as other tumor processes, provide maximum diagnostic information about the location, size, structure of the tumor, its relationship with the bone structures in the area of the temporal pyramid bones, intracranial cisterns and surrounding parts of the medulla (brain stem and cerebellum) in the intracranial space.
The combination of these methods allows you to make an accurate diagnosis of vestibular schwannoma and obtain all the data necessary for treating the patient, whether it is surgical treatment or radiological treatment (radiosurgery or radiotherapy).
On CT, the acoustic neuroma appears as an iso- or hypodense formation. The tumor stroma has a homogeneous or slightly heterogeneous density. The presence of fresh hemorrhages or calcifications in the tumor stroma is not typical. The exception is cases of cyst formation, as a result of impaired blood circulation in the tumor tissue.
A targeted CT scan of the temporal bone pyramid, performed in bone mode, reveals a cone-shaped expansion of the internal auditory canal with its base towards the intracranial space. In addition, CT scan of the temporal bone allows before surgery to determine changes caused by a tumor in the internal auditory canal, visualize the topography of the labyrinth, the dome of the jugular vein, and the degree of pneumatization.
MRI provides more information regarding the intracranial part of the tumor. About 2/3 of the tumors have a reduced density compared to brain tissue on T1 and 1/3 appear iso-density. MRI also provides adequate visualization of the structures of the labyrinth, the border of tumor spread in the internal auditory canal, the topography of the dome of the jugular vein, and in some groups of patients it is more preferable than CT for surgical planning.
Analysis of the rich clinical experience in treating patients with acoustic neuromas, which is not available in any neurosurgical clinic in the world, allowed us to identify three treatment options for this pathology:
- Observation;
- Removal of the tumor using a microsurgical method;
- Radiosurgery.
Diagnostics
-a picture of a small size acoustic neuroma after administration of a contrast agent.
Features -the picture of an acoustic neuroma depends on the size of the tumor. Neuromas less than 1 cm in size are difficult to detect. In the initial stages, the main methods are otoneurological examination and radiography of the temporal bones according to Stenvers. On radiographs, a sign of acoustic neuroma is dilation of the internal auditory canal. Up to 40% of tumors measuring 2 cm in diameter remain unrecognized on conventional CT without the introduction of contrast agents[30].
These tumors absorb contrast agents introduced into the blood well. In most cases, the X-ray density increases from 45 to 110 Hounsfield units. Neuromas typically have a round shape and smooth contours[30].
An MRI reveals an even contour of the tumor and along its periphery a signal strip of the so-called “cerebrospinal fluid gap”, deformation of the cerebellum and brain stem. When a neuroma spreads into the internal auditory canal, its extracanal part has the appearance of a “hanging drop” [30].
Approximately two-thirds of neuromas appear hypointense and one-third are isointense on T1-weighted scans. On T2-weighted tomograms, neuromas are characterized by an increase in signal, the degree of which varies. Areas of heterogeneously altered signal (due to the formation of cysts) are characteristic of large tumors (usually more than 3 cm). All neuromas intensively accumulate contrast agents, and in more than 70% of cases their accumulation is heterogeneous[30].
Treatment
Treatment of vestibular schwannoma has several directions:
- Drug treatment.
- Radiation therapy.
- Surgical treatment.
The conservative method of treatment is preferred when the acoustic neuroma is small in size, clinical symptoms are practically not manifested, and concomitant pathology or the patient’s advanced age do not allow surgery due to the risk to the patient’s life.
During this period, the patient is prescribed diuretics, non-steroidal anti-inflammatory drugs, painkillers, and complex supportive therapy for the underlying disease. During this period, the doctor observes the growth rate and location of the tumor, and the consequences of its growth. If symptoms begin to worsen, more aggressive treatment is decided.
The surgical method of treatment is radical and consists of performing a neurosurgical operation to remove the neuroma . This helps prevent hearing loss and sometimes even restore hearing.
The operation is performed under general anesthesia. To do this, an incision is made on the scalp, then a part of the bone is cut out and penetrated directly into the cranial cavity, the tumor is removed. Thanks to the latest developments in microsurgery, the surgeon’s movements practically do not touch or injure surrounding tissues. With small volumes of schwannoma, hearing is almost completely restored after surgery. If the acoustic neuroma is large, surgical access is carried out through the posterior cranial fossa. This greatly increases the risk to the life and health of the patient during surgery, since this method is more traumatic.
After the operation, the patient spends several days in the intensive care ward, then in the neurosurgery department. Full recovery occurs within a year. During this time, all the consequences of the operation appear, and the person returns to the normal rhythm of life.
Another effective treatment method is radiation therapy. With the development of microtechnology and improvement of knowledge, surgeons began to actively use the gamma knife.
Despite its effectiveness and high results, radiation therapy cannot be used as monotherapy; it only complements the operation to remove the tumor . It is used in two versions: as a preparation for surgical treatment to destroy schwannoma cells or after removal of the tumor to destroy the remaining cells.
During the procedure, the patient does not feel anything, it is non-invasive and completely painless. However, radiation therapy has a number of side effects: nausea, vomiting, lack of appetite, dermatological problems, hair loss, sometimes in the delayed period, paralysis and paresis of the facial nerve, hearing loss.
There is no specific prevention for acoustic neuroma. However, you can protect yourself by undergoing an annual medical examination and being observed by an ENT specialist, this is especially true for people with a family history of patients with acoustic neuroma.
Drug therapy
When a neoplasm in the auditory system is small, for example, when it is detected on brain images that were taken for other indications, oncologists do not immediately recommend removing the lesion. In the absence of pronounced negative symptoms, they recommend various medications. The purpose of the drugs is to improve the patient’s well-being, as well as help his body overcome the disease on its own.
As a rule, funds are selected from the following subgroups:
- diuretics - to eliminate excess fluid in the brain structures, reduce intracranial pressure;
- anti-inflammatory drugs - suppressing the manifestations of the inflammatory process in tissues, relieving pain;
- analgesics - overcoming pain that inevitably appears due to compression of brain structures;
- cytostatics are drugs that suppress the growth and development of tumor cells.
Diagnosis and treatment
The specialist must, first of all, study the history of the disease; an ENT examination of the ears and an examination of the patient’s nervous system are also carried out. There are also special diagnostic methods, including magnetic resonance and computed tomography, which make it possible to determine the presence of a tumor in the early stages. A pure-tone audiogram can help determine the functional state of hearing, and in case of a pronounced neuroma, electronystagmography can have a great effect. The final point of the examination is a face-to-face consultation with a neurosurgeon, who will decide on the method of treatment, although experts recommend removal of the acoustic neuroma in Burdenko. Feedback from patients suggests that the prognosis for surgical intervention at an early stage of the disease is positive.
Please note that removal of the acoustic neuroma can be done at the Burdenko Research Institute with A.G. Gavrilov.
Among the treatment options for the disease, watchful waiting tactics for monitoring the tumor, radiation therapy, external irradiation are considered, and recently radiosurgery is often used for this. The option for removing an acoustic neuroma and the cost of the operation depend on many factors, but this is often the only effective way to get rid of the problem. The operation is performed by three access options - rectosigmoid (without hearing damage), translabyrinthine (accompanied by hearing damage) and extradural infratemporal, which is performed through the midcranial fossa and is only possible when treating a small tumor.
As practice shows, removal of an acoustic neuroma has positive consequences in 95% of cases. The mortality rate is approximately 1%, and if the problem was managed at the initial stage of the disease, there is a high probability that hearing will be preserved. As for the advanced stages, in frequent cases not only hearing is lost, but also facial paralysis occurs. As you understand, the consequences will be less the sooner you seek help from a specialist.
It should be remembered that the treatment option depends largely on the location and size of the tumor. If we are dealing with a small tumor up to 10 millimeters in size, then the radiosurgery method works effectively; if the tumor reaches 10-20 millimeters, then it is better to resort to surgery, although radiosurgery is no less effective in this case. As for large tumors, there is no alternative to microsurgery. In some cases, doctors also resort to radiation therapy, which is used separately and in combination with surgery.
It is also important not only to diagnose acoustic neuroma in a timely manner, but also to take precautions after surgery. The recovery period lasts differently for everyone - for some, 2-3 weeks are enough to recover, for others it takes months to fully recover. A positive prognosis increases if symptoms were identified in the early stages and treatment was started in a timely manner.
MRI technique
No preliminary preparation is required before the MRI diagnostic procedure of the auditory nerve. The patient must be prepared to stay in the closed cylindrical chamber of the tomograph for about half an hour. When contrast agents are used, the patient should be evaluated for allergic reactions to certain substances administered intravenously. In case of fear of closed spaces, the patient takes several sedative tablets orally. They do not affect the overall picture obtained during diagnosis. Contraindications to the use of MRI may include electronic implants, such as pacemakers or hearing amplifiers. Dentures with a significant iron content can also be an obstacle. After the procedure, the patient receives the information obtained during the examination and its transcript within a few hours. Further interpretation of the data obtained and the prescription of appropriate treatment should be done by the doctor who referred the patient for examination. Making decisions on your own about taking certain medications is unacceptable.
Prevention
Sudden ear pain accompanied by hearing loss can be prevented by following a number of recommendations. Disease prevention means:
- Maintaining a healthy lifestyle, giving up bad habits;
- Strengthening the immune system;
- Wearing special equipment and headphones in the presence of harmful working conditions;
- Avoiding head injuries;
- Undergoing periodic preventive examinations, especially in the presence of serious chronic diseases.
And it is very important that when the first signs of auditory neuritis are detected, it is recommended not to self-medicate, but to immediately consult a doctor.
Disease prognosis
At stages 1 and 2 of auditory neuroma, the prognosis is very favorable - the slow benign growth of the lesion allows it to be diagnosed and eliminated in a timely manner. The five-year survival rate is about 80–90%.
When a patient presents with the third stage of a tumor defect, one should expect the formation of complications - paresis, paralysis of facial tissues, disturbances in facial expressions, and auditory/visual activity. The most unfavorable prognosis is for stage 4 of the disease, when distant secondary foci of cancer have already formed.
Specific prevention of the formation of auditory neuroma has not been developed, since the root causes of its development have not been definitively established. Experts include maintaining a healthy lifestyle with proper nutrition and adequate physical activity as methods of secondary prevention of pathology. Avoidance of individual bad habits, timely relief of neuroinfections and other somatic disorders contributes to the prevention of neuromas.
Postoperative period
After a large neuroma and removal of the nerve roots, loss of motor functions, facial expressions and hearing is possible. To restore partial sensitivity and normalize muscle tone in the postoperative period, massage is necessary. In case of significant impairments, the patient is given a disability group.
The risk of developing a neuroma after removal is reduced to zero. The life prognosis is favorable.
Tumors of the VIII pair of nerves (neurinomas) are located in the middle section of the pontocerebellar rocky space and can arise from the Schwann membrane along its entire length, from the bottom of the internal auditory canal to the entrance to the medulla oblongata. Let us recall that the pontocerebellar rocky space is topographically divided into three sections: anterior, middle and posterior.
Depending on which department the pathological process is located, a corresponding syndrome occurs. Tumors of the auditory nerve (neurinomas) are of great interest to otolaryngologists because the first complaints resulting from damage to the VIII pair of nerves (tinnitus, decreased hearing, static disturbances) force the patient to seek help from an otolaryngologist. Such patients, under the supervision of an otolaryngologist, are diagnosed with otosclerosis, inner ear disease, or Meniere's disease.
Consequently, otiatrists do not sufficiently differentiate between a tumor of the VIII pair of nerves and other diseases of the auditory nerve and inner ear of non-inflammatory origin. This is the main reason why the tumor. VIII pairs of nerves are recognized at a late stage of their development.
Neuroma in its initial development can sometimes occur without disruption of cochlear and vestibular function. This probably happens in cases where the tumor originates from the medial sections of the VIII pair of nerves. The first symptoms of medially located tumors are expressed in headaches, a feeling of tightness in the back of the head, neck, paresis of the facial nerve, taste disturbances, and facial pain reminiscent of neuralgia. With such a localization of the neuroma at the onset of the disease, noise in the ear and decreased hearing may be completely absent, or the change in hearing may be so insignificant that the patient does not notice it, and therefore does not complain of hearing impairment.
Such patients are usually not referred to an otolaryngologist for examination. When hearing impairment and stato-kinetics have reached a significant degree, only then are such patients referred by a neurologist to a specialist to establish dysfunction of the VIII pair of nerves. In order to avoid late recognition of damage to the auditory and statokinetic apparatus of a tumor nature, one should make it a rule to carry out an in-depth study of the function of the VIII pair of nerves in any disease of the nervous system.
.