Treatment approaches
Treatment should be aimed at eliminating the cause of the speech disorder and its correction. If an ischemic stroke is detected in a patient, thrombolytic therapy is administered with Actilyse and other similar drugs. If the stroke was hemorrhagic in nature, then hemostatic treatment is necessary. Neoplasms and hematomas are subject to neurosurgical removal or radiotherapy. If a bacterial infection is detected, antibiotics are prescribed (Amoxiclav, etc.).
Elimination of speech disorders is carried out using the following methods:
- Speech therapy exercises on a regular basis. The task of a speech therapist is to expand operational auditory-verbal memory to eliminate clinical manifestations. Such classes should be carried out from the first days of rehabilitation of patients with organic brain lesions. Initially, the exercises are easy, but their complexity gradually increases. The patient is given dictations, songs, poems, etc. are memorized. If the patient has difficulty finding words to express his thoughts, the speech therapist helps him by clarifying their meaning and systematization.
- Among medications, preference is given to medications that improve cerebral circulation (Vinpocetine, Actovegin), nootropics (Phenotropil, Piracetam) and neurometabolic agents (Gamma-aminobutyric acid).
In addition to these methods, psychotherapy, therapeutic massage, physiotherapeutic procedures (electrosleep, magnetic therapy) and other methods of rehabilitation are recommended.
With early initiation of speech therapy treatment and elimination of the causes of the development of acoustic-mnestic aphasia, the prognosis is favorable. A person’s speech skills are gradually restored, up to their previous level. If the patient has been self-medicating for a long time, and the underlying pathology has progressed significantly, then the effectiveness of therapy is limited.
Aphasia after stroke and more
Aphasia is most common in older people who have had a stroke
. However, speech destruction occurs in young people and even in children who have suffered infectious diseases, traumatic brain injuries, or brain tumors. The form of aphasia depends on which part of the brain is affected. And the direction in which speech restoration specialists will work depends on the form.
Diagnosis of aphasia
Experts from different fields are involved in uncovering the mechanisms of this complex disease: neurophysiologists, neurologists, speech therapists, psychologists, etc. The diagnosis is made after the localization of the lesion in the brain has been determined. The complexity of the disorder depends on the size of the lesion, the nature of the circulatory disorder and the characteristics of the intact components of speech activity.
It is known that the highest mental functions of a person are carried out as a result of the work of the cortex of the two hemispheres of the brain and its subcortical structures. Aphasia is caused by damage to the dominant hemisphere, the right in left-handed people and the left in right-handed people.
This is how the frontal lobes of the cortex carry out programming, regulation of mental activity and correction of its results. The right frontal lobe carries out non-speech actions, the left is responsible for the movement of the tongue and the entire body, plans speech and mental activity, and predicts its impact on the situation. The temporal lobes of the cortex are responsible for listening and understanding speech. The right temporal lobe captures and differentiates non-speech sounds, the left is responsible for the perception of both individual sounds of language and their synthesis into groups of words. The occipital lobes of the cortex perform the functions of collecting and processing information through vision, the parietal lobes - through the tactile-kinesthetic sense.
Diagnosis of the activity of cerebral cortex functions in aphasia is carried out in the following areas:
|
Main forms of aphasia
There are several classifications of aphasia; in our country, the classification of A.R. is widespread. Luria, abroad – Lichtheim-Wernicke classification. There is also a simplified classification: posterior form of aphasia - damage to the superior temporal and inferior parietal areas of the brain, and anterior form - damage to the posterior frontal regions. Classic descriptions examine not only lesions of the speech areas of the brain, but also adjacent non-speech areas of the cortex.
Features of the development of aphasia are different. In cases of circulatory disorders and brain injuries, speech disorder occurs sharply and immediately. With sluggish circulatory disorders and gradual growth of a brain tumor, the symptoms of aphasia appear slowly, as the brain zones are covered.
MOTOR APHASIA OF AFFERENT TYPE
Stage of severe disorders
1. Overcoming disorders of understanding situational and everyday speech:
- display of pictures and real images of the most commonly used objects and simple actions by their names, categorical and other characteristics. For example: “Show a table, a cup, a dog, etc.”, “Show pieces of furniture, clothing, transport, etc.” “Show someone who flies, who talks, who sings, who has a tail, etc.”
— classification of words by topic (for example: “Clothing”, “Furniture”, etc.) based on a subject picture;
— answers with an affirmative or negative gesture to simple situational questions. For example, “Is it winter now, summer..?”; "You live in Moscow?" and etc.
2. Disinhibition of the pronunciation side of speech:
- conjugate, reflected and independent pronunciation of automated speech series (ordinal counting, days of the week, months in order, singing with words, ending proverbs and phrases with a “hard” context), modeling situations that stimulate the pronunciation of onomatopoeic pronouns (“ah!” “oh” !" and so on.);
- conjugate and reflected pronunciation of simple words and phrases;
- inhibition of the speech embolus by introducing it into a word (ta, ta..-Tata, so), or into a phrase (ma..ma-mama...; this is mom).
3. Stimulating simple communicative types of speech:
— answers to questions in one or two words in a simple situational dialogue;
— modeling situations that contribute to the evocation of communicatively significant words (yes, no, want, will, etc.);
— answers to situational questions and composing simple phrases using a pictogram and a gesture accompanied by the pronunciation of simple words and phrases.
4. Stimulating global reading and writing:
— laying out captions under pictures (subject and subject);
- writing the most common words-ideograms, copying simple texts;
— conjugate reading of simple dialogues.
Moderate stage of disorders
1. Overcoming disorders of the pronunciation side of speech:
- isolating sounds from words;
— automation of individual articles in words with different syllabic structures;
— overcoming literal paraphasias by selecting first discrete and then gradually converging sounds in articulation.
2. Restoration and correction of phrasal speech:
- composing phrases based on a plot picture: from simple models (subject-predicate, subject-predicate-object) to more complex ones, including objects with prepositions, negative words, etc.;
- composing phrases on questions, on key words;
- exteriorization of grammatical-semantic connections of the predicate: “who?”, “why?”, “when?”, “where?” etc.;
— filling in gaps in a phrase with a grammatical change in a word;
— detailed answers to questions;
- compiling stories based on a series of plot pictures;
- retelling texts based on questions.
3. Work on the semantics of the word:
— development of generalized concepts;
- semantic play on words (subject and verbal vocabulary) by including them in various semantic contexts;
— filling in the gaps in a phrase;
- completing sentences with different words that are appropriate in meaning;
- selection of antonyms, synonyms.
4. Restoration of analytical-synthetic writing and reading:
- the sound-letter composition of the word, its analysis (one-two-three-syllable words) based on diagrams that convey the syllabic and sound-letter structure of the word, a gradual reduction in the number of external supports;
- filling in missing letters and syllables in words;
- copying words, phrases and small texts with an emphasis on self-control and independent error correction;>
- reading and writing from dictation of words with a gradually more complex sound structure, simple phrases, as well as individual syllables and letters;
- filling in missing words in texts when reading and writing, practiced in oral speech.
Stage of mild disorders
1. Further correction of the pronunciation aspect of speech:
— clarification with articles of individual sounds, especially affricates and diphthongs;
— differentiation of acoustic and kinesthetic images that are similar in articulation of sounds in order to eliminate literal paraphasias;
- practicing the purity of pronunciation of individual sounds in a sound stream, in phrases, with a combination of consonant sounds, in tongue twisters, etc.
2. Formation of detailed speech, complicated in semantic and syntactic structure:
- filling in the missing main sentence, as well as a subordinate sentence or subordinating conjunction in a complex sentence;
- answering questions with complex sentences;
- retelling texts without relying on questions;
— drawing up detailed plans for texts;
— preparation of thematic messages (short reports);
- speech improvisations on a given topic.
3. Further work to restore the semantic structure of the word:
- interpretation of individual words, mainly with abstract meaning;
— explanation of homonyms, metaphors, proverbs, phraseological units.
4. Work on understanding complex logical and grammatical figures of speech:
— execution of instructions, including logical and grammatical phrases;
— introduction of additional words, pictures, questions that facilitate the perception of complex speech structures.
5. Further restoration of reading and writing:
- reading and retelling expanded texts;
- dictations;
— written presentation of texts;
— writing letters, greeting cards, etc.;
- essays on a given topic.
1) Restoring the “articuleme-phoneme” connection
- writing letters corresponding to the names of sounds in expressive speech, reading these letters immediately after writing;
- isolating the first sound from simple words, fixing attention on the articulatory, acoustic, and then graphic image of this sound; independent selection of words for this sound and writing them;
- writing practiced sounds and syllables under dictation;
— identification of letters in different fonts;
— finding given letters in various texts (underlining, writing out).
2) Restoring the ability to sound-letter analysis of the composition of a word:
- dividing words into syllables, syllables into letters (sounds) based on various graphic schemes;
- highlighting any sound in a word;
- recalculation and listing of words by letter (orally);
- filling in gaps in words;
- writing words from letters given separately.
3) Restoring the skill of detailed written speech:
- writing words of different sound structures with and without support from an object picture: a) under dictation, b) when naming an object or action;
- writing proposals: a) from memory, b) from dictation, c) in the form of a written statement based on a plot picture for the purpose of communication with others;
- written statements and essays.
Classification
Aphasia is classified according to several criteria.
Depending on the location of the lesion, the following forms of pathology are distinguished:
- Afferent motor. Damage occurs to the lower parts of the postcentral cerebral cortex. With this type of disorder, a person cannot utter a word, since afferent aphasia causes a breakdown in connections between sound expressions and the articulatory apparatus. At the same time, the patient can involuntarily pronounce individual words or sounds, but is not able to do this at the request: he has no idea how to close or open his lips and in what position to put his tongue in order to pronounce a certain sound.
- Efferent. This form of disorder is caused by a pathological process in the lower parts of the premotor region. This zone is responsible for programming speech, that is, it causes the flow of one sound or syllable into another, resulting in the formation of words. The peculiarity of the efferent form of aphasia is that a person is able to pronounce individual sounds at will or at request, but cannot combine sounds into words to form a complete word.
- Acoustic-gnostic or sensory. The deviation is associated with damage to the upper part of the temporal region of the brain. This area is responsible for human perception and understanding of the auditory part of speech. As a result, the patient completely or partially loses the ability to understand and analyze speech addressed to him. At the same time, people with sensory aphasia do not have impaired physical hearing, they are able to put syllables into words and speak, they can easily pronounce simple and familiar words, but they cannot verbally reproduce unfamiliar and complex ones. With acoustic-gnostic aphasia, the patient's speech is very confused, and the structure of the composed sentence is incomprehensible to the listener.
- Acoustic-mnestic. Speech impairment is caused by damage to the middle temporal gyrus. The deviation is expressed in a violation of auditory-verbal memory. The patient is noted to be forgetful: he can know exactly the meaning of an object, but cannot name it in one word, while “sorting out” all its characteristics. Patients with acoustic-mnestic aphasia do not understand the meaning of antonyms and synonyms, they do not understand the figurative meaning of words, they have a vocabulary deficit, their speech is spontaneous, emotional, and consists mainly of verbs. Memory impairment leads to impairments in writing and understanding the text being read.
- Semantic. The disorder develops in the case of damage to the posterior temporal and anterior parietal parts of the cerebral cortex. The patient cannot compare time and space. He fully understands speech and speaks correctly, but in speech structures with such a deviation, logical connections are disrupted. Also, patients with semantic aphasia have a lack of understanding of the figurative meaning of words, sayings, and proverbs.
- Dynamic. This form of aphasia is associated with damage to the posterior frontal regions of the brain. The patient's communicative function of speech is impaired: his speech is scanty, spontaneous, and undynamic. The patient's remarks do not contain prepositions, verbs, or complex adjectives. Words and their grammatical forms of words do not agree with each other.
From a linguistic point of view, the following types of aphasia are distinguished:
- Verbal. In this case, we are talking about violations of word formation, the presence of pronunciation defects, and limited vocabulary.
- Nominal. This type of aphasia makes it impossible to perceive speech and use words.
- Syntactic. In this case, the patient loses the coherence of sentences and speaks in a telegraphic style.
- Semantic. A patient suffering from this type of aphasia has a distorted perception of the meaning of a grammatically complex structure.
Depending on the severity of the disorder, total and partial aphasia are distinguished. In the first case, there is a complete impairment of the patient’s speech, in the second – partial.
The severity of the speech disorder directly depends on the location of the lesion and its size.
Pathogenesis
Amnestic aphasia is provoked by dysfunction of the temporal and parietal areas of the brain cortex.
Medical experts once assumed that this anomaly does not occur in its pure form. In their opinion, amnestic aphasia should be considered a 1-stage manifestation of sensory and motor pathology. This is relevant in the presence of a tumor process in the GM, as well as regression of anomalies during vascular processes.
Amnestic aphasia is observed with damage to the temporoparietal region. The defect in this case is associated with difficulties that arise when a person tries to remember the name of a particular phenomenon or object. During the course of the anomaly, the presence of verbal paraphasias and amnestic relapses is noted.
Symptoms
Symptoms of sensory aphasia include typical neurological signs and psycho-emotional disorders, which are secondary and caused by the difficult situation in which the patient finds himself.
- Inability to perceive speech. With intact hearing (in most cases), a person cannot make out what others are saying. Speech is heard, but it is not understood. It was as if the patient was surrounded by foreigners. This is the most complex version of the disorder. In lighter forms, the ability to perceive some simple structures is retained. Monosyllabic or phrases.
- Inability to speak independently. There are different levels of speech impairment. In classic cases, a person is able to speak, but in short phrases or even individual simple words. At the same time, he poorly understands what he himself is saying. In the most advanced forms, total speech dysfunction is observed. The patient makes inarticulate sounds. Features of the speech of patients with sensory aphasia are fragmentation, lack of clear logical connections, and the most poor lexical and grammatical structure. Usually these are fragmentary words and phrases.
- Psychomotor agitation. Accompanied by increased physical activity. The patient rushes about, cannot find a place for himself. A panic attack is possible. Severe attack of fear, panic.
- Aggressiveness, hostility. Within the framework of preserved consciousness. The affect of anger is associated with anxiety and lack of understanding of what is happening. Assistance is required; if necessary, an injection of a sedative is prescribed.
Additional symptoms are usually not associated with sensory aphasia and have a concomitant neurological origin. These are epileptic seizures with impaired consciousness, convulsions, loss of visual acuity, disruption of normal visibility, loss of individual fields of vision (scotoma). Verbal hallucinations are also common. Pseudohallucinations, when a person hears voices in his head. Paradoxically, the patient is not able to interpret even imaginary hallucinatory images; they are felt as auditory stimuli of a speech nature with incomprehensible content.
Signs of sensory aphasia persist throughout most of the period of the pathological process.
Reasons for appearance
Dynamic aphasia appears in humans as a result of organic lesions of the cortex of the speech centers of the brain. All factors that contribute to the development of pathology develop in the patient with already formed speech. The etiology of aphasic deviations always leaves an imprint on the patient’s prognosis for recovery, as well as on his character and course of the disease.
One of the reasons, although not the most common, is vascular diseases of the brain, namely ischemic or hemorrhagic strokes. As for patients who have suffered a hemorrhagic stroke, they more often suffer from mixed or total aphasic syndrome. If we are talking about the occurrence of ischemic abnormalities in the blood circulation, a motor or sensory form of pathology occurs.
Use an Adsense clicker on your websites and blogs or on YouTube
Common causes that lead to dynamic aphasia include the following:
- Any traumatic brain injury.
- Inflammatory pathologies of the brain, namely encephalitis, abscess or leukoencephalitis.
- Neoplasms of the brain.
- Chronic diseases that are in the progress stage.
- Deviations of the central nervous system.
- Surgical intervention.
How severe the disease will be depends on the location of the main problem area
The etiology of the speech disorder and the extent of the lesion are also taken into account. As for the onset of the disease due to a brain tumor, aphasic disorder will manifest itself gradually, but as for stroke or TBI, the development occurs abruptly
If we talk about intracerebral hemorrhage, it is always accompanied by more severe disorders of the speech apparatus than, for example, in the case of thrombosis or atherosclerosis. The age of the patients plays a fundamental role in the recovery process. The younger the patient, the greater his chances for a faster and more complete recovery due to the extensive compensatory potential.
Causes
The syndrome is based on lesions in the cerebral cortex. Dysfunction of the departments and death of neurons can result from the following situations:
- hemorrhages;
- malignant and benign tumors;
- operations in brain structures;
- TBI;
- neuroinfections;
- stroke;
- blows, head bruises;
- Alzheimer's disease;
- multiple sclerosis;
- peak hormonal states (pregnancy, puberty, menopause).
Localization of the lesion occurs when there are structural changes in the TPO zone in the area of the dominant hemisphere. The central mechanism for the development of the disease becomes a violation of the perception of sound, image, and space.
Correction methods
The main corrective intervention with which the disorder can be cured is considered to be medical and speech therapy.
The first step is to treat the disease that caused the development of the disease. This occurs under the careful supervision of a neurologist or neurosurgeon. In this case, drug treatment can be used, in some cases surgery, after which active rehabilitation begins (that is, the use of mechanotherapy, physiotherapy and massage).
Speech restoration occurs in classes with a speech therapist; the method used by the specialist is selected based on the type of deviation and etiology.
The best effect will be noticeable if correctional work begins immediately after a stroke or injury. But the start of classes, first of all, must be agreed with a doctor. Thus, there will be an obstacle to the recording of speech pathologies. The period of such work may take from two to four years.
The prognosis for the restoration of speech functioning depends on how quickly the correction began, on the location of the lesion, the age of the patient and on the state of health in general.
If there is a spontaneous recovery from motor aphasia, the person develops stuttering.
In order to prevent the formation of aphasia, it is necessary to monitor the health of cerebral vessels, avoid traumatic brain injuries and the development of inflammatory processes. The most important thing to remember is that only through the joint efforts of specialists and family members will it be possible to restore the patient after such a serious speech disorder.
Diagnosis of pathology
If the patient shows the first signs of dynamic or mnestic aphasia, it is necessary to conduct a series of studies that will confirm or refute the presence of pathology, as well as determine the degree of severity. Not a single diagnostic measure can be performed without these tests, since speech functions may not be completely lost. To determine the nature of the problems encountered, the patient is asked to do the following:
- Writing a summary based on the text read.
- Compose an essay on the proposed topic.
- Description of the plot of the picture seen.
- Compose a story in your own words based on the images provided.
Based on the test results, the patient’s degree of proficiency in his inner speech will be assessed, since some types of aphasia, in particular dynamic, leave certain speech functions that can be preserved in the future.
If the patient has not experienced problems with counting or writing up to this point, these abilities will most likely not be affected. The main abilities that will remain in a functioning state include the following:
- the ability to identify phenomena and objects and name them;
- the ability to repeat word forms, speech patterns and cliches after the interlocutor;
- the ability to name the order of months, years, days of the week, and also use speech nearby.
DYNAMIC APHASAIA
Stage of severe disorders
1. Increasing the level of general activity of the patient, overcoming speech inactivity, organizing voluntary attention:
- performing various types of non-verbal activities (drawing, modeling, etc.);
— assessment of distorted images, words, phrases, etc.;
- situational, emotionally significant dialogue for the patient;
- listening to plot texts and answering questions about them in the form of affirmative-negative gestures or words “yes”, “no”.
2. Stimulating simple types of communicative speech:
— automation in dialogical speech of communicatively significant words: “yes”, “no”, “can”, “want”, “will”, “must”, etc.;
— automation of individual cliches of communicative, incentive and interrogative speech: “give”, “come here”, “who’s there?”, “hush!” etc.
3. Overcoming speech programming disorders:
- stimulation of answers to questions with a gradual decrease in the answer of words borrowed from the question;
- constructing phrases of the simplest syntactic models based on chips and a simple plot picture;
- performing simple grammatical transformations to change words that make up a phrase, but are presented in nominative forms;
- laying out a series of sequential pictures according to the plot contained in them.
4. Overcoming grammatical structuring disorders
5. Stimulating written speech:
— laying out captions under pictures;
- reading ideogram words and phrases.
Moderate stage of disorders
1. Restoration of communicative phrasal speech:
— construction of a simple phrase;
- composing phrases based on a plot picture using the chip method and gradually “collapsing” the number of external supports;
- compiling a story based on a series of sequential pictures;
— detailed answers to questions in the dialogue;
- compiling simple dialogues like speech sketches: “In a store” - a dialogue between a buyer and a seller, “In a savings bank”, “In an atelier”, etc.
2. Overcoming perseverations in independent oral and written statements:
- display of objects in pictures and in the room, parts of the body (in random order, by individual names and by series of names);
- ending phrases with different words;
- selection of words of given categories and in given quantities, for example, two words related to the topic “Clothing” and one word related to the topic “Tableware”, etc.;
- writing numbers and letters broken down (from dictation);
- writing from dictation of words and phrases that contribute to the development of semantic and motor switching;
— elements of sound-letter analysis of the composition of a word: folding simple words from letters of a split alphabet;
- filling in gaps in words;
- writing simple words from memory and dictation.
Stage of mild disorders
1. Restoration of spontaneous communicative phrasal speech:
- extensive dialogue on various topics;
- constructing phrases based on a plot picture with a gradual decrease in the number of external supports;
— automation of phrases of certain syntactic models in spontaneous speech;
- accumulation of a verbal dictionary and “revitalization” of the semantic connections behind the predicate (with the help of questions posed to it);
- reading and retelling texts;
- “role-playing conversations”, playing out a certain situation;
- “speech improvisations” on a given topic;
- detailed presentations of texts, essays;
- drafting greeting cards, letters, etc.
Diagnostic measures
Diagnosis of the acoustic-mnestic form of aphasia requires the participation of different specialists and a set of studies. The patient should be consulted by a neurologist, psychiatrist, speech therapist, aphasiologist, and neuropsychologist. Based on the collected anamnestic data, a diagnosis is made.
Neurological examination
The neurological basis of the diagnosis is the identification of pathology of the cranial nerves, the presence of spastic hemiparesis, and impaired reflexes. A cognitive examination is also carried out to rule out mental disorders.
Speech examination
Features of speech activity are identified by a speech therapist and aphasiologist.
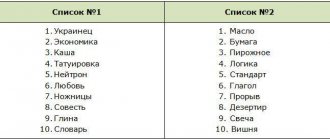
When examining a patient with acoustic-mnestic dysfunction, verbal paraphasia, dyslexia, dysgraphia, and agrammatisms in speech will be detected. Experts will also pay attention to the level of auditory-verbal memory. The patient is asked to remember and reproduce a chain of ten short words that are not related to each other
Often the subject remembers only 1 word from the proposed ones, the last one.
Another task: 2 groups of lexical series of 3 words each are given. They also need to be remembered and retold. Most often, patients fail to cope with the task: they group words incorrectly and find it difficult to remember what exactly was called.
To examine auditory-verbal memory for a text, you are asked to listen to a short passage, retell it and answer questions. To record optical-gnostic disorders, the patient is asked to draw, for example, a cup or a teapot. If there is a pathology, the images will be missing details: a handle or spout.
Brain MRI
Magnetic resonance imaging will show the presence of tumor formations, foci of inflammation, degenerative changes, and traumatic injuries.
Vascular studies
To study blood vessels, ultrasound, duplex scanning, and MR angiography are prescribed. These studies make it possible to confirm or refute cerebrovascular pathology. They also show the characteristics of cerebral, collateral circulation, and the presence of vascular occlusion.
Lumbar puncture
To check for suspected neuroinfection, a lumbar puncture is performed. During the procedure, cerebrospinal fluid is taken from the patient. Laboratory examination of the material will show whether an inflammatory process is present, determine the pathogen, the presence of cancer cells, and signs of hemorrhage.
Differential diagnosis
When examined superficially, symptoms of acoustic-mnestic disorder can be confused with signs of other speech disorders
Therefore, it is important to pay special attention to collecting anamnesis
Thus, the difference between this type of aphasia and motor one lies in the activity of spontaneous speech. In acoustic-gnostic aphasia, as opposed to mnestic aphasia, the utterance is less complete and there are literal paraphasias. It is also necessary to distinguish between aphasia and cognitive impairment.
Symptoms
It doesn’t matter what type of aphasia is formed, as a result of any one, a general speech disorder appears. This happens due to the loss of any speech side, which subsequently causes a secondary collapse of the entire speech system
People who suffer from aphasia have a “telegraphic style” of speech, that is, long pauses and hypophonia are heard in pronunciation. The development of alexia and agraphia also begins.
Afferent motor aphasia can manifest itself in two ways.
- In the first type, the formation of articulatory apraxia, the absolute disappearance of spontaneous speech, as well as the appearance of speech repetition are observed.
- In the second type, conduction aphasia develops, situational speech is present, and disturbances in repetition and arbitrary naming occur.
Acoustic-gnostic (sensory) aphasia is accompanied by damage to the perception of auditory information when the hearing aid is in a completely healthy state. The patient is unable to perceive the speech of other people, and there is also a lack of control over the flow of words.
The development of acoustic-mnestic aphasia is characterized by the inability to retain in memory information that has been heard. When working with a speech therapist, the patient cannot repeat after the specialist a link that consists of three or four words.
Amnestic-semantic aphasia manifests itself in the form of memory loss for the names of elementary objects. This aphasia is rare in children and is most often observed among older people. The perception of complex speech is impaired, including the lack of understanding of proverbs or metaphors, as well as popular expressions. There is an inability to understand the text that has been read.
With the development of the dynamic type, the patient is able to correctly pronounce only individual sounds, short phrases and words.
Treatment
Treatment of amnestic-semantic aphasia must be comprehensive. In this case, one should not hesitate, since the sooner corrective measures are started, the greater the patient’s chances of restoring lost cognitive functions.
After a diagnostic examination and clarification of the severity of damage to the speech centers of the brain, specialists formulate an individual treatment plan. In drawing up a treatment plan, in addition to functional and organic disorders, the patient’s age and mental state play an important role. Both a neurologist and a psychotherapist must work with each patient to achieve maximum effectiveness from therapy. If a serious organic pathology is detected that requires immediate surgical treatment, for example, in case of brain injuries or tumor lesions, emergency or planned surgical intervention is performed to eliminate the life-threatening condition and minimize cognitive impairment in the future.
Step-by-step rehabilitation
Restoring cognitive abilities is a rather long stage, requiring motivation and effort, both from the patient himself and from his relatives.
The rehabilitation period occurs individually for each patient and depends on many factors. However, a properly formed step-by-step plan can speed up recovery efforts.
At the initial stage, the victim is re-taught to adequately perceive objects and imaginative thinking. The patient constantly works with pictures of objects, then with groups of objects with a gradual complication of the visual series.
The second stage is to form adaptation to situational speech. The maintenance of speech function on certain topics is formed. At this stage, the patient requires the help of a speech therapist and psychotherapist, since it is the most difficult.
At the final stage, the patient expands his reserve of speech and auditory perception, and also learns to reduce the intervals between spoken phrases and sentences. A gradual increase in the volume of perceived information finally leads to adaptation of a person with aphasia.
Clinical Brain Institute
Rating: 4/5 — 3 votes
SENSORY APHASIA
Stage of severe disorders
1. Accumulation of everyday passive vocabulary:
— display of pictures depicting objects and actions by their names, functional, classification and other characteristics
— display of pictures depicting objects belonging to certain categories (“clothing”, “dishes”, “furniture”, etc.);
- showing body parts in the picture and in yourself;
- choosing the correct name of the object and action among the correct and conflicting designations based on the picture.
2. Stimulation of understanding of situational phrasal speech:
- answering questions with words “yes”, “no”, affirmative or negative gesture;>
- following simple oral instructions;
— capturing semantic distortions in simple phrases deformed in meaning.
3. Preparation for restoration of written speech:
— laying out captions for subject and simple plot pictures;
— answers to questions in a simple dialogue based on visual perception of the text of the question and answer;
- writing words, syllables and letters from memory;
- “voiced reading” of individual letters, syllables and words (the patient reads “to himself”, and the teacher reads out loud);
- development of the “phoneme-grapheme” connection by selecting a given letter and syllable by name, writing letters and syllables under dictation.
Moderate stage of disorders
1. Restoration of phonemic hearing:
- differentiation of words that differ in length and rhythmic structure;
- highlighting the same 1st sound in words of different lengths and rhythmic structures, for example: “house”, “sofa”, etc.;
- highlighting different 1st sounds in words with the same rhythmic structure, for example, “work”, “care”, “gate”, etc.;
- differentiation of words that are similar in length and rhythmic structure with disjunctive and oppositional phonemes by identifying differentiated phonemes, filling in gaps in words and phrases; capturing semantic distortions in a phrase; answers to questions containing words with oppositional phonemes; reading texts with these words.
2. Restoring understanding of the meaning of a word:
— development of generalized concepts by classifying words into categories; selection of a generalizing word for groups of words belonging to one or another category;
— filling in gaps in phrases;
- selection of definitions for words.
3. Overcoming oral speech disorders:
— “imposing a framework” on a statement by composing sentences from a given number of words (instructions: “Make a sentence of 3 words!”, etc.);
— clarification of the lexical and phonetic composition of the phrase using the analysis of verbal and literal paraphasias admitted by the patient;
— elimination of elements of agrammatism using exercises to “revitalize” the sense of language, as well as analysis of grammatical distortions.
4. Restoration of written speech:
- strengthening the “phoneme-grapheme” connection by reading and writing letters under dictation;
— various types of sound-letter analysis of the composition of a word with a gradual “collapse” of external supports;
- writing from dictation of words and simple phrases;
- reading words and phrases, as well as simple texts, followed by answers to questions;
- independent writing of words and phrases from pictures or written dialogue.
Stage of mild disorders
1. Restoring understanding of extended speech:
— answers to questions in an expanded, non-situational dialogue;
- listening to texts and answering questions about them;
— capturing distortions in deformed compound and complex sentences;
— understanding of logical and grammatical figures of speech;
— implementation of oral instructions in the form of logical and grammatical figures of speech.
2. Further work to restore the semantic structure of the word:
- selection of synonyms as homogeneous members of a sentence and out of context;
- work on homonyms, antonyms, phraseological units.
3. Correction of oral speech:
— restoration of the self-control function by fixing the patient’s attention on his mistakes;
- compiling stories based on a series of plot pictures;
- retelling texts according to plan and without plan;
— drawing up plans for texts;
- composing speech improvisations on a given topic;
— speech sketches with elements of “role-playing games”.
4. Further restoration of reading and writing:
— reading expanded texts, various fonts;
- dictations;
- written statements;
- written essays;
- mastering samples of congratulatory letters, business notes, etc.
Diagnostics
Amnestic aphasia is a disease that lies at the intersection of two areas: neurology and psychology. Since aphasia is characterized by various disorders of the cognitive function of the brain, such disorders cannot but be accompanied by mental defects. Neuropsychological diagnostic methods are used to identify amnestic aphasia. To verify the disease and clarify the degree of impairment of the functional activity of the speech apparatus of a sick person, they resort to the use of special tests. Typically, such tests use a variety of objects with varying degrees of difficulty in pronouncing their names. There are also tests of a descriptive nature, when the patient is told about the characteristics of an object and see if the patient can answer with hints. A number of tests determine the connection between speech and visual manifestations, for example, the patient is sequentially shown several objects belonging to the same category; if the patient does not respond, then he has a violation of the connection between speech function and visual images, which can be interpreted in favor of sensory-amnestic aphasia.
In addition to special neurological and psychological tests, each patient is required to undergo laboratory and instrumental research methods. Depending on the cause of aphasia, diagnostic methods will be more or less informative.
The Clinical Brain Institute has a high-tech diagnostic department, which can conduct research such as:
- Tomographic studies: computed tomography and magnetic resonance imaging with and without contrast;
- X-ray examination of the skull and brain to identify defects;
- Ultrasound sonography and Doppler mapping of neck vessels;
- Comprehensive laboratory diagnostics.
What is amnestic aphasia
All types of aphasia arise as a result of a decrease in the functionality of the tissues of the cortex or brain substance at the location of the sections responsible for the formation of speech. This can occur under the influence of external factors, internal processes, and organic lesions of the central nervous system. Amnestic aphasia becomes the result of disorders that span the border at the junction of the temporal, parietal and occipital regions in the left hemisphere of the brain. As is clear from the name of the pathology, it occurs with certain manifestations of amnesia.
Amnestic aphasia is considered one of the mildest speech disorders. Its course is accompanied by a minimal loss of control by the patient over the higher functions of his nervous system. The clinical picture of the pathology is quite vague, sometimes the patient and his relatives do not even notice the presence of problems. The disorder is characterized by a loss of the ability to quickly select words for verbal expression of thoughts. During spontaneous speech, the patient forgets the names of objects, but can describe them. This to some extent complicates his interaction with others.
With amnestic aphasia, the victim’s articulation is not impaired and the level of intelligence is not reduced. He retains his usual hearing acuity. From the outside, the presentation of information by such a person looks somewhat strange. He uses few nouns, chooses verbs poorly, and operates mainly with lengthy descriptions.
During spontaneous speech, the patient forgets the names of objects, but can describe them.
Diagnostics
Diagnosis is carried out in a hospital setting. At the initial stage, an initial examination by a neurologist is indicated. Since the patient cannot answer questions, the presence of a relative or someone who can answer some questions for the patient is desirable, but this is not necessary. Typical primary signs are also noticeable: anxiety, excitability, misunderstanding of speech, difficulties with speaking.
A routine neurological examination is mandatory. The simplest basic reflexes are tested.
As part of the assessment of the general condition, the severity of damage to cerebral structures, and the nature of such, a group of instrumental measures is prescribed.
MRI is the basis and gold standard for diagnosis. Aimed at visualizing neural tissue. Allows you to diagnose all structural disorders. If necessary, targeted tomography of individual areas of the brain is prescribed. Especially the temporal lobes. Gadolinium contrast enhancement is often used. The drug accumulates in the changed tissues and enhances the pattern. Contrast is indispensable when diagnosing tumors. Infrequently, sensory aphasia is also possible with multiple sclerosis, which will also be clearly visible on post-contrast images in all details. For high-quality diagnostics, you need a high-field device with a power of 1.5 Tesla. If possible. Low-field ones will provide less data.
MRI of the brain
If vascular neoplasms are detected, angiography is additionally performed to better visualize the disorder.
Dopplerography of the neck vessels and duplex scanning of the brain are mandatory to assess the degree of blood flow in the cerebral structures. This will allow you to detect cerebrovascular insufficiency and assess its severity.
Specialists whose help will also be required are a neurosurgeon, a vascular surgeon. The characteristics of sensory aphasia within a specific medical history should be as detailed as possible in order to determine the type of pathological process and its features. Without this, there can be no effective treatment.
ACOUSTIC-MNESTIC APHASIA
Stage of disorders of moderate and mild severity
1. Expanding the scope of auditory perception:
— display of objects (real and in pictures) by name, presented in pairs, triplets, etc.;
- showing body parts according to the same principle;
— implementation of 2-3-level oral instructions;
— answers to detailed questions, complicated by syntactic structure;
- listening to texts consisting of several sentences and answering questions about the content of the texts;
- writing from dictation with a gradual increase in phrases;
- reading gradually increasing phrases, followed by reproduction (from memory) of each of the sentences and the entire set as a whole.
2. Overcoming weakness of auditory-speech traces:
- repetition from memory of read letters, words, phrases with a gradual increase in the time interval between reading and reproduction, as well as filling the pause with some other type of activity;
— memorizing short poems and prose texts;
— repeated display of objects and pictures after 5-10 seconds, after 1 minute. after the first presentation;
- reading texts with time-delayed retelling (after 10 minutes, 30 minutes, the next day, etc.);
- composing orally sentences using reference words perceived visually;
- listing words by letter with a gradually more complex sound structure, and gradually moving away from the written example of these words.
3. Overcoming naming difficulties:
- analysis of visual images and independent drawing of objects denoted by name words;
- semantic play in contexts of various types of words denoting objects, actions and attributes of objects;
— classification of words with independent finding of a generalizing word;
— exercises on the interpretation of words with concrete, abstract and figurative meaning.
4. Organization of a detailed statement:
- compiling a story based on a series of plot pictures;
- retelling of texts, first according to a detailed plan, then according to a condensed plan, then without a plan;
- extensive dialogues on non-situational topics (professional, social, etc.); practicing samples of communicative and narrative writing (greeting cards, letters, statements, essays on a given topic, etc.).
Treatment approaches
Effective therapy is based on eliminating the immediate cause of the development of speech disorder. If a tumor lesion or intracranial hematoma is detected, treatment is carried out with neurosurgery, radiation or chemotherapy. Neuroinfections are eliminated using antifungal, antibacterial or antiviral drugs. Strokes are subject to thrombolytic or hemostatic treatment.
Correction of speech disorders is based on the use of two approaches:
Use of medications
Drug therapy improves the condition of the nervous tissue. For this purpose, several groups of drugs are used: nootropics (Glycine, Cortexin), vascular-active drugs (Cerebrolysin, Vinpocetine) and neuroprotectors (Gamma-aminobutyric acid). Additionally, Memantine can be used.
These medications have a positive effect on metabolic processes inside neurons, improve their recovery and functioning. For severe depressive disorder, antidepressants are prescribed (Amitriptyline, Fluoxetine, etc.). Any drug is used only as prescribed by the attending physician. All medications have indications and contraindications, non-compliance with which may cause the progression of the underlying disease or the development of side effects.
Regular speech therapy sessions
They are carried out to increase the volume of auditory-verbal memory. They must be started immediately after the onset of the disease, without delaying a visit to a speech therapist for the rehabilitation period. Initially, exercises with visual perception of an object are used, which makes them easier to remember. Next, the specialist complicates the lessons - the patient writes simple dictations by ear, learns fragments of sentences, word chains, songs and poems. To improve expressive speech, active work is being carried out to clarify the meaning of words and systematize them into separate groups.
In parallel with the treatment of the main pathology, rehabilitation measures begin with the patient. An important part of therapy is communication with medical staff, speech therapist and loved ones. As a result of constant verbal contact and speech therapy exercises, auditory-verbal memory is restored. In addition, patients are advised to exercise therapy, massage and visit a psychotherapist.