Brain death
- a condition when the death of the brain occurs, while with the help of resuscitation measures the function of the heart, blood circulation and respiratory activity are artificially maintained, creating the appearance of life. Currently, “brain death” is understood as a pathological condition associated with total necrosis of the brain, as well as the first cervical segments of the spinal cord, while maintaining cardiac activity and gas exchange, ensured by continuous artificial ventilation.
Brain death can be due to many reasons, including brain injury, intoxication, and swelling of the brain due to other causes.
Necrosis of the first cervical segments is caused by cessation of blood circulation through the vertebral artery system.
The actual synonym for brain death is the concept of “exorbitant coma,” the treatment of which is meaningless. A patient who is declared brain dead is actually a “living corpse.” In the practice of pathologists, the term “respiratory brain” is sometimes used. The condition must be distinguished from a chronic vegetative state.
Content
- 1 Criteria for brain death 1.1 Russia
- 1.2 United States of America 1.2.1 Ophthalmic examination
- 1.2.2 Lack of motor response to severe, deep central pain
- 1.2.3 Absence of complicating diagnoses and conditions simulating brain death
- 2.1 Cerebral angiography
- 3.1 Brain death in Christianity
Criteria for brain death
Russia
According to the order of the Russian Ministry of Health[1], the following signs indicate brain death:
- Complete and persistent lack of consciousness (coma).
- Atony of all muscles.
- Lack of response to strong painful stimuli in the area of the trigeminal points and any other reflexes that close above the cervical spinal cord.
- Lack of pupil reaction to direct bright light. It should be known that no medications that dilate the pupils were used. The eyeballs are motionless.
- Absence of corneal reflexes.
- Absence of oculocephalic reflexes.
- Absence of oculovestibular reflexes.
- Absence of pharyngeal and tracheal reflexes.
- Lack of spontaneous breathing.
USA
According to the recommendations of the US Presidential Commission[2], the following signs indicate brain death:
Ophthalmological examination
- “fixed pupils”: lack of pupillary response to light.
- Absence of corneal reflexes.
- Absence of the oculocephalic reflex (“doll eyes”).
- Lack of swallowing reflex.
- Absence of oculovestibular reflex (caloric test with ice water). The external auditory canal of one ear is washed with 60-100 ml of ice water (not performed if the eardrum is damaged) with the head raised 30° above the horizontal plane of the bed. Brain death is excluded if, in response to rinsing with ice water, the eyeballs turn towards the ear being rinsed. The procedure is repeated on the other side no less than 5 minutes after the previous examination.
- Apnea test: absence of spontaneous respiratory movements when the patient is disconnected from the ventilator (to determine the function of the medulla oblongata). An increase in the partial pressure of CO2 in arterial blood leads to an increase in intracranial pressure, which in turn can cause cerebral hernia and vasomotor instability, so this test should be performed last, when the causes of brain death are obvious.
- PaCO2 should be above 60 mmHg, and the absence of breathing confirms the diagnosis of brain death. The test is not evidence-based in patients with chronic obstructive pulmonary diseases and chronic heart failure.
Hypoxemia during the test should be excluded (due to the risk of developing cardiac arrhythmia and myocardial infarction). For this:
- Before the procedure, the lungs are ventilated with 100% oxygen for 15 minutes.
- Before the test, the patient is transferred to artificial ventilation, maintaining PaCO2 > 40 mmHg (this shortens the test time and makes it possible to more confidently avoid hypoxemia).
- During the test, passive oxygen inhalation should be performed at a rate of 6 l/min through a catheter for suction from the tracheostomy tube.
- It begins with normocapnia, the average time to reach the level of PaCO2 = 60 mmHg is 6 minutes (which corresponds to the classic growth rate of hypercapnia -3.7 +/-2.3), sometimes it is necessary to wait up to 12 minutes. The test should be interrupted if: the patient is breathing (does not meet the definition of death).
- severe arterial hypotension develops.
- Oxygen saturation drops below 80%.
- Severe cardiac arrhythmia develops.
If the patient is not breathing, arterial blood is sent to determine blood gases at regular intervals, regardless of the reasons that led to the termination of the test. If PaCO2 > 60 mmHg and the patient is not breathing, the test is considered positive. If the patient's condition is stable, determination of blood gases takes a few minutes, and PaCO2 < 60mmHg, the test can be continued.
Lack of motor response to severe, deep central pain
- The presence of decortication or decerebrate postures, as well as seizures, excludes the diagnosis of brain death.
- Presence of spinal reflexes (abdominal and cremasteric reflexes can be observed in brain death).
Absence of complicating diagnoses and conditions simulating brain death
- Hypothermia: Core body temperature should be greater than 32°C.
- Data on potentially reversible endogenous and exogenous intoxications, including those of drug and metabolic origin (barbiturates, benzodiazepines, meprobamate, methaqualone, trichloroethylene, paralyzing drugs, hepatic encephalopathy, hyperosmolar coma). If there is any doubt, laboratory testing of blood and urine for drug content is necessary.
- Shock (systolic blood pressure should be greater than 90 mmHg) and anoxia.
- Immediately after resuscitation (fixed and dilated pupils may be a result of atropine use).
- Patients after barbituric coma (the content should not exceed 10 mcg/ml).
- Confirmation of the diagnosis of brain death (EEG, cerebral angiography, cerebral isotope angiography, auditory evoked potentials of the brainstem are not performed, but may be considered appropriate by the consulting therapist).
- In cases of extensive brain damage due to irreversible pathological processes (massive cerebral hemorrhage and the like), some experts may make a diagnosis of brain death based on a single examination and confirmation by clinical confirmatory tests.
- For undoubted irreversible, clinically established conditions and the use of clinical confirmatory tests after 6 hours.
- In cases of undoubted irreversible, clinically established conditions and in the absence of clinical confirmatory tests after 12 hours.
- In case of inaccurate clinical diagnosis and in the absence of clinical confirmatory tests - 12-24 hours.
- In case of anoxic brain injury as the cause of brain death - 24 hours, but the observation period can be shortened when determining the cessation of cerebral blood flow.
Neural sculpture: how the brain changes throughout life and why age is not a barrier to learning
The human brain consists of tens of billions of neurons. As they grow up, they connect into a large-scale network that changes throughout their lives under the influence of the external environment. This plasticity makes it possible to improve cognitive abilities in adulthood, recover from serious injuries, and solve the most unexpected problems.
T&P publishes an excerpt from a book by contemporary philosopher Catherine Malabou about why the brain resembles a sculpture, how certain activities help improve memory, and whether there are limits to plasticity.
1. Developmental plasticity: formation of neural connections
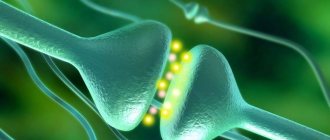
[…] “The human brain,” says Jean-Pierre Changer, “appears to us as a gigantic assembly of tens of billions of neural “webs” entangled with each other, where thousands of electrical impulses “chirp” and spread, here and there intercepted by a wide range of chemical signals."
These “webs,” also called “ramifications,” are neural connections that gradually form as an individual develops. When they talk about plasticity, it is this neurogenesis that is characterized. The brain essentially shapes itself. “A person is born with a brain that weighs 300 grams, that is, five times less than an adult brain... One of the main features of the development of the human brain is that it continues for a long time after birth... approximately fifteen years.” So it all starts with making connections, then multiplying them and making them more complex. The increase in brain mass coincides with the growth of axons and dendrites, the formation of synapses, and the development of myelin sheaths around the axons. This development is subject to strict genetic determinism. In their origin and structure, “all human brains are similar to each other,” says Marc Jeanreau. Of course, the connections that make up the anatomy of the mature brain are not a matter of chance or spontaneous organization. The migration of nerve cells and their adaptation to final goals are programmed. “We’ll give just one example,” the author continues. - In all people, the fibers emanating from the retina and carrying visual information complete their path in the visual part of the cerebral cortex, that is, in the occipital lobe, located in the back of the brain; in all people, this visual part forms connections with other areas located in the parietal, temporal lobe, etc. Consequently, the adult brain reflects the existence of a pre-established plan, which ensures the invariance of anatomy from one individual to another.”
If neurogenesis follows a “preset plan,” why even talk about plasticity to characterize this development? For two significant reasons related to 1) the aforementioned process of connection establishment and 2) their formation (which is different from modulation of synaptic effectiveness). In both cases, the execution of the program acts as plastic. There is, so to speak, a plastic art of the brain, which explains the use of the term “plasticity” in this context. It is here that the narrowed or “closed” meaning of this concept—sculpture of a predetermined form—comes to the fore.
In the process of making connections, a sculptor's chisel can be compared to a phenomenon called apoptosis, or cell death. This death is a normal occurrence. It again corresponds to the execution of a genetic program, which leads to the elimination of useless connections and the gradual formation of the final form of the system by targeting nerve fibers to target cells. In the human brain, neuronal death begins at the end of the fetal period and continues through at least the first six months of life. In an adult, its dynamics slow down significantly. As Jean-Pierre Changet writes: “The destruction of neurons is part of normal development. It constitutes one of its decisive stages.” In a book with the eloquent title “The Sculpture of the Living,” biologist Jean-Claude Amaisen emphasizes the fact that the brain, far from being, as has long been assumed, a fully formed organ at birth, is an institution that simultaneously takes and gives itself its own form. “Cell death,” he writes, “is ... a tool that allows the embryo to develop its form by a method of elimination, which makes it similar to sculpture.”
Meanwhile, as Marc Genreau explains, from this stage of development and as soon as the system takes on a complete sculptural form, “genetic determinism weakens.” “After birth, the topographic network, formed during embryogenesis and stabilized through the death of neurons and the elimination of connections, begins to function under the influence of external factors. This functioning entails a new phase of joint formation.” The environment plays a fundamental role here.
Much of the development of the human brain occurs in open space, in contact with stimuli from the world, which directly affect the growth and volume of connections.
For example, the visual system is not fully functional at birth. The synapses that connect fibers emanating from the retina to neurons in the visual cortex are not yet fully formed. And it is information received from the outside that activates these synapses and promotes their maturation. It is in this vein that it is customary to talk about the formation of synapses or the mechanism of synaptic plasticity (as we see, still associated with the genetic program) in the second phase of development.
The process of brain formation during these two phases - the establishment of connections and their maturation under the influence of the environment - thus reveals plasticity in the execution of the program. In both cases, the brain appears as formed - gradually sculpted, stabilized, divided into different regions - and at the same time as a formative authority: little by little, as the volume of connections increases, the identity of the individual is drawn. And the further we go, the more this “first plasticity” loses its inexorable determinism. The sculptor gradually begins to improvise. Our own activity plays an increasingly important role in shaping connections: “Our brain, shaped by our own activities, our interactions with the outside world, as well as the influences we experience during our upbringing, knows our history and life path. From this proximity is born a deep identity of the functioning of our brain and our understanding of the world, one might even say an identity of views.”
In fact, the first level of plasticity is closely related to the second, since the influence of the environment gradually replaces epigenetic “sculpting” and becomes more and more pronounced. The narrowed or “closed” meaning of plasticity very soon comes across its “open” meaning - “freedom”, in which determinism and uncertainty surprisingly converge. And indeed, we see that brain morphogenesis does not lead to the establishment of a rigid and finally fixed structure, but to the formation of what can be called a template. It is then honed (sculpted) during development and then - to a lesser extent, but with no less efficiency - throughout life. The neural activity of pre-established circuits thus replaces the sculptured activity of apoptosis. From now on, the role of morphogenic factors is played by the environment of the brain as an organ (formation of connections), and then by its external environment (synaptic modulation under the influence of the environment).
Source: Svetlana Mokrova / istockphoto.com
Modulation plasticity: the brain and its history
At this point we immediately encounter the second field of action of neuroplasticity - the modification of neural connections through modulation of synaptic effectiveness. Undoubtedly, it is at this level that plasticity manifests itself with the greatest brightness and strength, and it is here that it “reveals” its meaning. In fact, there is a kind of neural “creativity” that does not depend on anything other than the individual’s experience, life and interactions with the environment. This “creativity” is not assigned exclusively to the human brain, but is already characteristic of the most rudimentary nervous systems.
This plasticity, which involves shaping branching patterns and modulating synaptic efficacy, was first identified by Canadian neurologist Donald Olding Hebb. In the late 1930s, various experimental observations led him to move away from the concept of rigid localization of memory chains in accordance with Pavlov's reflex arc model. In his opinion, one should rather talk about the existence of “plastic synapses” capable of adapting their transmission efficiency. Hebb formulated the hypothesis of neural circuits capable of self-organization, that is, modification of their connections during the activities necessary for perception and learning. The synapse is the primary site where neural activity can leave a trace that can displace, change, or transform itself through the repetition of past actions.
The ability of synapses to modulate their effectiveness and modify the intensity of their branches under the influence of experience occurs in two directions. Either the effectiveness of the synapse (its ability to transmit signals from neuron to neuron) increases - this is “long-term potentiation (LTP or LTP)”; or it decreases - this is “long-term depression (LTD or LTD).” This can already be seen in the example of such an animal as Aplysia. Its central nervous system is simple and consists of eight pairs of ganglia located around the esophagus and a large abdominal ganglion. Aplysia has a meager set of behavioral stereotypes, among which a number of defensive maneuvers can be distinguished, such as retracting the siphon or gills. At the same time, the strength of her protective reflex is modulated by experience. Repeating non-hazardous stimulation on the mantle causes a decrease in the reflex (habituation), which is expressed in a decrease in the amplitude of retreat movements. Habituation is accompanied by suppression of synaptic activity and a proportional decrease in the amount of neurotransmitter released at the level of the sensory-motor synapse.
The phenomena of long-term potentiation and depression are even more clearly expressed in the processes of adaptation, learning and memory in birds. For example, the black-capped chickadee stores food in pantries, which it then unerringly finds. Researchers were able to establish that the size of the brain area (hippocampus) involved in this process is larger in this bird than in others that do not have experience storing food. Therefore, species that practice storage have a significantly larger hippocampus in comparison with others. This change is a consequence of the accumulation of new neurons, decreased cell death (apoptosis), and increased connections between hippocampal neurons. The latter thus demonstrates amazing structural plasticity.
Potentiation and depression are not simply synaptic processes during which one or more stimulations produce immediate excitation. These are also long-term modifications that can transform the form (changes in the size of a certain brain area, varying the permeability of a regularly excited area) and remove a trace in order to reapply it (lability of the memory trace). Indeed, it has been observed that some neural networks become more productive when they “suppress” synapses that were involved in tasks that led to errors in motor learning. In the human brain, this feature is clearly evident during all learning processes. For example, when learning to play the piano, a mechanism for suppressing input signals corresponding to erroneous movements (“misses”) makes it possible to learn correct movements. In the case of potentiated connections, synapses increase the area of contact, their permeability increases, and nerve conduction accelerates. Conversely, a synapse that is underused or "suppressed" tends to become less productive. Neurons store stimulation impulses in some way. It is as if the stabilization of memories occurred solely under the condition of a potential destabilization of the overall landscape of memory.
So, long-term potentiation is structurally related to long-term depression, and this connection constitutes the differentiating, or rather transdifferentiating, force of neuroplasticity. If we use the analogy with the formation of stem cells, we can assume that, due to their plasticity, neural connections are always able to change a difference, perceive an imprint or get rid of it, and transform their program.
Hence,
The fact that synapses show increased or decreased effectiveness as a function of experience suggests that, although the anatomy of the brain is the same in all people, no brain is identical in history to another.
This is directly evidenced by the phenomena of learning and memory. Repetition and habit play an essential role, which means that the neural chain never has a clearly fixed response. Plasticity combines the role of the sculptor with the functions of the artist and educator of freedom and autonomy. In a sense, it is plausible to say that synapses represent the brain's reserves for the future. They are not fixed and do not serve as mere transmitters of neural information, but they have the power to shape or reform that information itself. Marc Genreau writes: “The effectiveness of synapses varies depending on the flow of information that passes through them: each of us, in childhood and throughout our lives, experiences a unique configuration of environmental influences that is reflected in the shape and function of our brain networks.”
This once again calls into question the old dogma that the adult brain tends to lose its plasticity - it is, of course, able to accumulate new information, but there is no change in its learning, memory functions and global structure, except perhaps to the side. decline or degeneration. On the contrary, we see that there is a constant restructuring of neural morphology.
3. Restorative plasticity: the brain and its regeneration
Here we come to consider the third field of action of plasticity - restoration. The term "restorative plasticity" actually refers to two different processes: neuronal renewal, or secondary neurogenesis, and the brain's ability to repair some types of damage caused by injury.
What is meant by “neuronal renewal” or “secondary neurogenesis”? From what we have just said, it appears that the first plasticity, morphogenetic, is followed by modulation plasticity, which modifies synaptic effectiveness but does not affect the anatomical stability of the brain, as if it were operating, so to speak, within a closed system. According to Heather Cameron: “Some scientists still adhere to the stable brain hypothesis, according to which there is no anatomical plasticity of the adult brain, and especially the cerebral cortex; They believe that the functional plasticity underlying learning mechanisms involves changes in the “power” of synapses produced by modification of receptors or the intercellular environment of neurons at the molecular level.” However, this dogma of a stable brain is not entirely true. Indeed, the author continues,
“We now know that individual neurons in areas important for learning are constantly being updated—and this amounts to relatively significant anatomical changes.”
Even if the role of stem cells in the adult brain and their localization are still poorly understood, and even if there is a possibility that secondary neurogenesis does not affect all regions of the brain, it is undeniable that nerve cells are renewed in adulthood. This opens up unprecedented prospects for brain restoration and changes our understanding of its functioning.
A recent study of the primate neocortex revealed the presence of new neurons in three regions of the association cortex: the prefrontal, inferior temporal, and parietal areas. “This result is particularly interesting because the association cortex plays an important role in high-level cognitive functions, while the striate cortex [which does not show updating] is involved in processing visual information. This difference suggests that while neurogenesis plays a key role in functions that are inherently plastic, it is not beneficial for lower-level functions such as sensory processing, which are typically stable throughout life.”
The production of new neurons is thus not simply about replacing dying cells. It plays a role in the plasticity of modulation and, because of this, further expands the concept of plasticity - to the point of shaking the concept of stability. Again: the statue comes to life, the program becomes animated. Where, as it seems to us, there is only pure mechanics, we find a complex interweaving of different types of plasticity, contradicting the usual ideas about the brain as a machine. As Alain Proshyants states: “It must be said that one of the main characteristics of the nervous system, of course, lies in its plasticity. The brain cannot be viewed as a network of finally laid cables, and brain aging cannot be viewed as the disconnection of an ever-increasing number of elements of this chain from the network. Even though this has only been formally proven in a few experimental models, we have the right to assume that nerve fibers grow daily, that some synapses disintegrate, while others, new ones, are formed. These changes in the neural landscape... are a testament to our adaptability, our ability to learn, and our potential for improvement, which continues into old age and, in fact, until death.”
In a paper titled “The Unusual Distribution of New Neurons,” the researchers state: “…observations of secondary neurogenesis clearly show that the adaptive capabilities of the nervous systems of birds and adult mammals do not arise solely from variability in synaptic connections. They also rely on the production or renewal of distinct populations of neurons in several highly defined regions, the common property of which is to perform functions responsible for learning and/or memory. In this light, it appears that secondary neurogenesis similarly allows the subject's personal experiences to leave their mark on neural networks in the form of regular morphological and functional rearrangements. This means that adult neurogenesis, as the ultimate mechanism of plasticity, largely controlled by the subject’s personal experience and its interactions with the environment, apparently constitutes an additional mechanism of individuation. With the significant difference that it lasts throughout life.”
The idea of cellular renewal, regeneration, resource as an aid to synaptic plasticity sheds light on the power of healing - healing, healing, compensation, restoration, the brain's ability to create natural "prostheses". The plastic art of the brain gives birth to a statue capable of healing itself. The functioning of the brain, as we know, can be impaired due to many pathologies, the most famous of which are traumatic brain injuries, cerebrovascular accidents, encephalitis, neurodegenerative diseases (Parkinson's disease, Alzheimer's disease). At the same time, after such injuries and illnesses, the nervous system invariably shows plasticity, regardless of whether its efforts are crowned with success or not: the affected structures and functions try to modify themselves in order to compensate for the deficiency or form a new organizational pattern that simultaneously deviates from the norm and restores it .
Restorative plasticity obviously does not compensate for all deficits. Some lesions, as we know, are irreversible. But at first, the brain always tries to reorganize the affected function with greater or less effectiveness, efficiency and reliability.
As an example of this phenomenon, Marc Janreau cites “paralysis of the left arm caused by damage to the motor cortex on the right due to a stroke. At first, no movement is possible, the hand is motionless and lethargic. After some time, muscle strength returns and mobility of the elbow and wrist is restored. How is this possible if the neurons responsible for controlling these movements are destroyed?... Here functional neuroimaging comes to the rescue: it shows that when the patient tries to move the paralyzed arm, it is the unaffected motor cortex on the left that is activated. The patient, either by himself or through rehabilitation, learns to use neural pathways that normally do not exist. Such a reorganization of motor function once again indicates the plasticity of cerebral mechanisms.”
Another example is what happens in the early stages of Alzheimer's disease. The onset of amnesia is partially compensated by the ability to restore stored information. The deactivation of some regions (hippocampus) is balanced by the metabolic activation of others (frontal). Thus,
damage to individual circuits is followed by a change in information processing strategies, which also indicates functional plasticity of the brain.
So, the human brain has functions responsible for reorganization after damage. These phenomena are also observed in some transplants. In January 2000, staff at the Edouard Herriot Hospital in Lyon performed the first hand transplant on thirty-three-year-old Denis Chatelier, who had suffered an amputation after an accidental explosion three years earlier. The question was: even if it is possible to establish anatomical continuity between the donor's hands and the recipient's forearms, can the same continuity be achieved at the psychological and neurological levels? The case of D. Sh. proved that yes. His phantom pain disappeared, and the motor progress he made suggested that his brain had successfully integrated the transplanted arms.
“When the motor cortex reorganizes, the synapses are modified. They change their influence and “weight” in the local functioning of the network of neurons... After transplantation, [such] changes in neural connections could lead to the restoration of the representation of the hand.”
Another proof of the amazing adaptability of our brain.
If you find an error, please select a piece of text and press Ctrl+Enter .
Share
Clinical confirmatory studies
Cerebral angiography
Nowadays it is rarely used due to the high cost, the need for transportation to the radiology department, the involvement of highly qualified workers, the waste of time and the potential danger of damage to organs intended for transplantation. Visualization of the absence of cerebral blood flow incompatible with brain life on angiography of 4 cerebral vessels is the Gold standard for brain death.
Electroencephalography - EEG
Can be performed at the patient's bedside[3]. Requires the participation of a qualified specialist - an interpreter. Does not detect brain stem activity. Electrocerebral silence (ECS) does not exclude the possibility of reversible coma. It is necessary to continue monitoring the patient for at least 6 hours after determining ECS. EEG can be used to clarify the diagnosis of brain death in patients in whom drug intoxication, hypothermia or shock have been reliably excluded. The definition of electrocerebral silence on the EEG is based on the absence of electrical activity > 2 microvolts under the following conditions:
- Recording electrodes from the scalp and neutral (referential) electrodes should be located at a distance of more than 10 cm
- Recording was carried out from 8 electrodes on the scalp and one on the ear
- Resistance between electrodes is less than 10,000 ohms (or impedance less than 6,000 ohms) but more than 100 ohms
- Sensitivity 2 µV/mm
- Time constants for parts of recording 0.3-0.4 sec (time constants for part of recording)
- Lack of response to stimuli (pain, noise, light)
- Recording over 30 min
- Repeated examination in doubtful cases
- Qualified technician and electroencephalographer with experience in intensive care units
- Transmission of EEG by telephone is unacceptable.
Cerebral radioisotope angiography - Cerebral Radionuclid Angiogram (CRAG)
Can be performed on a bed using a conventional scintillation chamber with a low energy collimator. May be ineffective in the presence of minimal cerebral blood flow, especially to the brainstem, so it is recommended to continue observation for 6 hours if there is no clear evidence of massive brain damage (trauma, hemorrhage) and other complications. The examination is carried out by an experienced interpreter.
Can be used to diagnose brain death in the following conditions:
- In the presence of conditions complicating the diagnosis - hypothermia, drug intoxication (patients brought out of a barbituric coma), metabolic disorders.
- In patients with massive facial trauma, when ophthalmological examination is difficult or doubtful.
- In patients with severe chronic obstructive pulmonary disease (COPD) or chronic heart failure (CHF), when the apnea test cannot be considered reliable.
- To shorten the observation period, especially when there is a question about organ transplantation.
Technique:
- The scintillation chamber is placed above the head and neck in an anteroposterior projection
- 20-30 mCi 99m Tc labeled albumin or pertechnetate in a volume of 0.5-1.5 ml is injected into a peripheral or central vein, followed by 30 ml of saline.
- A series of dynamic images are taken at 2-second intervals for 60 seconds.
- Then a statistical analysis of images of 400,000 counts is carried out in the anteroposterior and then in the lateral projection.
- If the examination needs to be repeated for reasons of questionable results or inconsistency with the diagnosis of brain death, this may be possible after a 12-hour interval necessary to remove the isotope from the circulating blood.
The study confirms that brain death demonstrates the absence of blood flow in the carotid arteries at the base of the skull, the absence of filling of the middle and anterior cerebral arteries (with brain death, delayed and true visualization of the dural sinuses may be observed). The absence of the “candelabra effect” indicates a lack of cerebral blood flow over the base of the brain.
Types of diagnostics
Brain atrophy is diagnosed using instrumental analysis methods.
Magnetic resonance imaging (MRI) allows you to examine in detail changes in the cortical and subcortical substance. Using the obtained images, it is possible to accurately make an appropriate diagnosis already in the early stages of the disease.
Computed tomography allows us to examine vascular lesions after a stroke and identify the causes of hemorrhage, determine the location of cystic formations that interfere with normal blood supply to tissues.
The newest research method - multislice tomography allows you to diagnose the disease at an early stage (subatrophy).
To determine after which cases of atrophied areas of brain tissue appear, diagnostic studies are prescribed. The difficulty of diagnosing in the early stages prevents correct, timely treatment and full restoration of functions. During the examination, the doctor determines the level of reflexes and reactivity - the ability to respond to external stimuli. Instrumental and hardware methods:
- MRI, CT. Allows you to identify cystic and tumor formations, hematomas, and local lesions.
- Ultrasound, neurosonography - in newborns.
- Dopplerography. Reveals the condition and patency of elements of the vascular system.
- Angiography is an X-ray examination of blood vessels.
Neurophysiological studies, including electroencephalography (determining the degree of brain activity), rheoencephalography (determining the state of cerebral circulation), diagnostic punctures, are carried out to identify the causes that led to damage to the cells that make up the brain tissue.
Brain death and religion
Brain death in Christianity
The Catholic Church considers the cessation of activity of the cerebral cortex to be a criterion for determining a person’s death[4].
In the Orthodox Church there is no clear opinion on whether brain death, given the functioning of other body systems, is the basis for declaring the fact of a person’s death. Death in Orthodoxy, based on Holy Scripture, is understood as the separation of the soul from the body (Ps. 146:4; Luke 12:20). Thus, theologian V.V. Zenkovsky writes that “the destruction of the body takes away from the soul the basis of its life (there is no brain, no nervous system, through which the soul receives material for life)”[5]. Therefore, artificial maintenance of the vital activity of the organism is considered appropriate only when there is hope for the continuation of life and functioning of the organism as a whole [6]. For this reason, in case of brain death, it is allowed to stop artificial ventilation [7].
Brain death in Islam
In many Islamic countries, the concept of brain death is used as a criterion for determining the death of the body, and after it it is allowed to stop intensive care[7]. This decision is based on the results of the Third International Conference of Islamic Jurists (1986) and the Fourth Session of the Council of the Islamic Academy of Jurisprudence (1988), which allowed the removal of organs from a person after brain death [ source not specified 3243 days
].
Brain death in Judaism
There is no consensus in Judaism on this issue. There are many points of view, of which the main three are the following[8][9][10]:
- The opinion is that it’s all about the activity of the heart. According to this point of view, a heart transplant may kill both the donor and the recipient, since the beating heart is removed from them. Currently, it is legal to accept donated organs[11][12].
- The opinion is that all life is in the brain, so while it is not obvious that the entire brain has decomposed, the possibility remains that the person is alive.
- Brain stem death is recognized as brain death, equivalent to the Talmudic case of immediate death upon decapitation[13]. The Israeli rabbinate has supported this point of view, and a bill is being prepared that brain death will be determined by a commission of doctors, lawyers and specially trained representatives of the rabbinate for rabbinic supervision independent of organ transplantation [ source not specified 3243 days
].
Causes of neuron death
The reasons for the death of brain cells can be different. The main processes that can cause the death of neurons:
- vascular accidents (heart attack, stroke);
- neuroinfections;
- toxic effects;
- traumatic lesions;
- hereditary predisposition.
Important! The death of nerve cells in the brain of unknown cause is called idiopathic.
Scientists believe that diseases based on the death of brain cells are an epidemic of the 21st century. Globally, diseases that develop as a result of the death of neurons can be:
- acute (stroke, encephalitis, traumatic brain injury);
- chronic (encephalopathy, multiple sclerosis, neurodegenerative diseases).
However, the term “brain death” is most often used in cases of neurodegenerative diseases. The main representatives of this group are:
- Parkinson's disease;
- Alzheimer's disease;
- Huntington's chorea;
- some forms of dementia;
- certain types of epilepsy;
- supranuclear gaze paresis.
Notes
- Order of the Ministry of Health of the Russian Federation No. 460 of December 20, 2001 On approval of instructions for ascertaining the death of a person based on a diagnosis of brain death
- President's Commission for Study of Ethical Problems in Medicine;
Guidelines for the Determination of Death . JAMA 246:2184-6, 1981. - Video demonstration “Confirming brain death using EEG”, youtube.com
- The Vatican has explained what is meant by “death” (undefined)
(unavailable link). Retrieved March 25, 2010. Archived October 20, 2010. - Zenkovsky V. Apologetics
- Fundamentals of the social concept of the Russian Orthodox Church Archived on August 24, 2013.
- ↑ 12
Perspectives from the world's major religions on end-of-life decisions in the intensive care unit - Encyclopedia of Jewish Medical Ethics, MD Avraham Steinberg
- “Defining the Moment of Death,” a collection of articles in Hebrew from the Assia magazine at the Institute of Medical Ethics at Shaare Zedek Hospital inaccessible
link). Retrieved March 25, 2010. Archived April 16, 2010. - Jewish Medical Ethics series (2 volumes) ditors
:
Rabbi Mordechai Halperin
, MD, Prof.
Shimon Glick
, MD, and
Rabbi David Fink
, PhD, “Determining the moment of death” (English)
(undefined)
(unavailable link). Retrieved March 25, 2010. Archived March 30, 2010. - "Tzitz Eliezer", b. E. Waldenberg
- “Minchat Yitzchak”, R. Yitzchak Yaakov Weiss
- R.'s opinion Moshe Feinstein in Igrot Moshe, revealed by the author's son-in-law R. Moshe David Tendler.
- American biotechnologists are learning to resurrect people from the dead
- Vegetative state. Treatment » Neurological portal :: Big Medical Portal