Affective-respiratory attacks in children (ARP, breath-holding spells) are a problem that raises numerous questions among parents. Few parents will tell you that they are unfamiliar with children's tantrums. Stomping feet, falling on the floor, crying and screaming in a crowded place, especially when refusing to buy a toy, candy, or chewing gum. However, the list can be continued endlessly. When faced with such paroxysms for the first time (this is another name for attacks), especially with blueness or convulsions, mothers and fathers fall into serious panic.
What are they?
Affective attacks in children are a short-term, lasting several seconds, cessation of breathing at the height of strong crying, accompanied by blue or pale skin. Against the backdrop of an emotional situation, an outburst of anger, the child begins to cry. Suddenly, the roaring baby becomes silent, turns blue, and goes limp due to a drop in muscle tone. This state usually lasts no more than a minute. Then the child behaves as usual. In some cases, there may be convulsive twitching, followed by weakness. This is the so-called blue attack.
There are white paroxysms. They develop in response to some kind of injury: he fell, hit his head, immediately turned pale and lost consciousness. At this moment, breathing also stops. The duration of such an ARP also does not exceed 30–60 seconds. Afterwards drowsiness appears.
Approaches to parenting if your baby has ARP
Affective-respiratory syndrome in children occurs due to nervousness. Therefore, in order for the baby to feel better, you need to pay attention to his psychological state. We must approach raising a child with full responsibility:
- You shouldn't pamper him too much; he should know that there are things in the house that shouldn't be touched.
- But you also can’t be too strict with your baby. We must remember that he is still small, and his psyche is just developing. Constant bans have a bad effect on him.
- It is best if the baby has his own corner or room where he can do everything, but only within its boundaries.
- The relationship between parents is also important. You can’t sort things out in front of children. The loud screams of adult babies frighten them, and they begin to cry. Fear can also lead to an attack with respiratory arrest.
A properly structured daily routine plays an important role. A well-rested and timely fed baby is less capricious and balanced than a tired and hungry one.
Where do they come from?
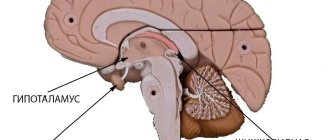
For a long time, ARPs were viewed as a manifestation of hysteria. Only the age of the patients, as well as years of observation, did not confirm this theory. Neurologists have found that, against the background of crying, a spasm of the muscles of the larynx occurs, leading to cessation of breathing. At an older age, a child may experience hysterical attacks in the classic version.
You need to be able to distinguish ARP from apnea syndrome, which occurs in premature or low birth weight babies, as well as in babies with diseases of the nervous and cardiovascular systems. This condition is a risk factor for sudden death syndrome. ARPs themselves do not pose a danger, but in the future they are a prerequisite for the development of epilepsy. It is impossible to deny the fact that moments of lack of breathing lead to oxygen starvation of the brain, which cannot but affect its functioning. In addition, ARP deplete the nervous system, which will subsequently cause memory and mental disorders.
Affective-respiratory convulsions and their difference from epileptic seizures
In order to be sure that your child's seizures are not a sign of developing epilepsy, you should have a good understanding of the differences between them.
- ARVs tend to become more frequent if the child is tired, and with epilepsy, an attack can develop in any condition.
- Epileptic seizures are the same. And affective-respiratory paroxysm occurs in different ways, depending on the severity of the situations that provoke it or the pain sensation.
- ARP occurs in children no older than 5-6 years, while epilepsy is a non-age disease.
- ARP is well affected by sedatives and nootropic drugs, but epileptic seizures cannot be stopped with sedative drugs.
- In addition, when examining a child with ARP, EEG results do not show the presence of epiactivity.
And yet we repeat: if twitching occurs during an attack of breath holding, parents should show the baby to the doctor.
How not to confuse it with other problems?
To distinguish hysterical attacks in a 2-year-old child from ARP, it should be taken into account that the latter are a clear protest against the parents’ refusal to fulfill any desire or prohibition from doing what they love. Hysterics are not accompanied by loss of consciousness or loss of muscle tone. They last longer and are intended to attract maximum attention from others - the child cries, stamps his feet, etc.
According to foreign researchers, ARPs are accompanied by a decrease in hemoglobin and a decrease in iron content in the blood. This is not a specific manifestation of attacks, but can aggravate the hypoxic effect on the brain.
Treatment of ARP
Drug treatment for seizures is extremely rare.
The decision for this is made by the doctor; under no circumstances should you drug the child yourself. Sedatives, vitamins and neuroprotectors are used for treatment. For about 2 months, the child is given Phenibut, Pantogam, Glycine or other similar medications. For sedatives, it is better to use herbal teas and baths. In rare cases, tranquilizers are prescribed - Grandaxin, Atarax and others.
If your baby easily tolerates attacks and recovers from them on his own, there is no need to panic and resort to medications. Most likely, over time, everything will work out for the baby without this.
Diagnostic search
For diagnosis, or rather to distinguish ARP from other seizure-like conditions, in particular from epilepsy, electroencephalography (EEG) is used. This is a technique for recording bioelectric potentials of the brain.
EEG is a highly accurate way to distinguish true epileptic seizures from seizures of other types, including ARP. In modern clinics, it is possible to record indicators of physiological brain activity around the clock simultaneously with video surveillance. Along with EEG, electrocardiography is required to exclude heart diseases leading to respiratory arrest, as well as spirography, a method that allows one to clarify the cause of respiratory arrest. Such an examination is necessary in cases where there is doubt about the origin of the seizures or the description provided by the parents is not clear enough.
Stopping breathing due to spasm of the muscles of the respiratory tract occurs with bronchial asthma and the entry of a foreign body. In these conditions, a cough with attacks of suffocation is observed in the child, while, against the background of prolonged paroxysm, there may be severe expiratory shortness of breath (on exhalation). Here you cannot do without a targeted consultation with a pulmonologist and allergist.
What to do during an attack?
First of all, don’t panic yourself. The emotional state of the surrounding adults is transmitted to the baby, and if confusion and fear are “stirred up,” it will only get worse. Hold your breath yourself. Feel that nothing bad happened to you and your baby due to the temporary delay in breathing movements. Blow on the baby's nose, pat his cheeks, tickle him. Any such impact will help him quickly recover and breathe.
During a prolonged attack, especially with convulsions, place the baby on a flat bed and turn his head to the side. This will prevent him from choking on vomit if he vomits. Spray him with cold water, wipe his face, and gently tickle him.
If during an attack parents “tear out their hair,” then the baby’s condition becomes more serious. After an attack, even if there were convulsions, give the baby a rest. Don't wake him if he's asleep. It is important to remain calm after an attack, speak quietly, and not make noise. In a nervous environment, the attack may recur.
For any attack with convulsions, you should consult a neurologist. Only a doctor can distinguish ARP from epilepsy or other neurological disorders.
Make an appointment with your doctor if this happens for the first time. It is necessary to distinguish between illness and affective reaction. If the attack has happened more than once, but there is no illness, you need to think about raising the baby.
If this happens to your baby for the first time, you should call a pediatric ambulance, especially if convulsions occur. The pediatrician will assess the severity of the condition and decide whether hospitalization is required. After all, parents are not always able to fully monitor their baby, and this is how the consequences of a traumatic brain injury, poisoning or acute illness can manifest themselves.
Simple rules for parents
The task of parents is to teach the child to manage his anger and rage so that it does not interfere with the lives of the rest of the family members.
Discontent, anger and rage are natural human emotions; no one is immune from them. However, boundaries must be created for the baby, which he has no right to cross. To do this you need this:
- Parents and all adults living with the child must be united in their requirements. There is nothing more harmful for a child when one allows and the other forbids. The child grows up to be a desperate manipulator, from whom everyone then suffers.
- Place in a children's team. There, the hierarchy is built naturally, the child learns to “know his place in the pack.” If attacks occur on the way to the garden, you need to consult a child psychologist, who will specifically indicate what needs to be done.
- Avoid situations where an attack is likely to occur. The morning rush, a queue at the supermarket, a long walk on an empty stomach - all these are provoking moments. It is necessary to plan the day so that the baby is well-fed, has sufficient rest and free time.
- Switch attention. If a child bursts into tears and the crying intensifies, you need to try to distract him with something - a passing car, a flower, a butterfly, snowfall - whatever. It is necessary not to let the emotional reaction “flare up” .
- Clearly define boundaries. If a child knows for sure that he will not receive a toy (candy, gadget) from either his grandmother or aunt, if his father or mother forbade it, then after the most desperate crying he will still calm down. Everything that happens needs to be spoken in a calm tone. Explain why crying is useless. “Look, no one in the store is crying or screaming. It’s impossible - it means it’s impossible.” Sensitive children need to add that mom or dad loves him very much, he is good, but there are rules that no one is allowed to break.
- Call a spade a spade and pronounce the consequences of whims. “You're angry and I can see it. But if you continue to cry, you will have to calm down alone in your room.” You need to be honest with children.
Treatment and behavior correction
Treatment of affective-respiratory attacks, like the treatment of any other disease, should be comprehensive and include both medicinal and non-medicinal methods. Correction of this pathology lies within the competence of a pediatric psychoneurologist, and timely redirection to a specialist directly depends on the pediatrician. Sedatives and drugs are prescribed to normalize the processes of excitation and inhibition. The child does not require special emergency measures (artificial respiration or spraying with water). The attack goes away on its own. Moreover, your actions may seriously frighten the baby.
How should parents behave during ARP?
In the course of ongoing scientific research, scientists have found that the parents of 25–27% of children suffering from ARP have had similar attacks in the past. But this does not at all indicate that attacks are inherited. Most likely, it is more appropriate in this case to talk about the traditions of upbringing in a family where two generations - parents and children - at one time suffered from the same problem. As a rule, doctors agree that the main factor causing the beginnings of childhood hysteria in the form of ARP can be considered conflicts between parents, stressful situations for the child in the family, and excessive parental care.
An affective-respiratory attack is mainly a neurotic disorder, so parents should pay priority attention to unobtrusive correction of the child’s psychological worldview.
When you somehow witness ARP in your child, it is advisable to immediately think about how you build a relationship with your child. Perhaps you are overprotective of him, sometimes trying to protect him from minor life adversities, or are you pampering him too much when parents do not deny their child anything? Here you may need to contact a psychologist if there is no mutual understanding between the spouses in your family.
The correct daily routine, which is based on a balanced, correct physical and mental load, is of great importance for the development of a strong child’s psyche. It will not be amiss if you closely monitor your baby during the day - this way you can predict and prevent the development of ARP. For example, a hungry and tired child will be more capricious than one who was fed and put to bed on time. This also applies to everything else: getting ready for kindergarten, going to visit or to the store - everything should cause the baby the least discomfort.
You definitely need to talk to the little man about his feelings. Indeed, in some cases, hysterics appear and continue to occur with enviable regularity only because the child cannot cope with his feelings and stop in time. But you just help the capricious person understand that all his emotions - anger, frustration, resentment - are completely natural, and they can be dealt with one way or another. Be sure to teach your child the art of compromise, because this can later help him out more than once in the future.
In case of particularly severe attacks of breath holding, the doctor may prescribe a course of treatment for the baby using neuroprotectors and sedatives (Pantogam, Glycine, Pantocalcin) lasting 1.5–2 months.
If the mother can prevent the child from approaching that dangerous edge beyond which whims and hysterics begin, it is quite possible to do without drug treatment.
Normalization of the psychological climate
Considering the immaturity of the physiological processes that regulate excitation and inhibition in the nervous system, it is necessary to take measures aimed at developing the child’s skills to control emotions. The baby is unable to express emotions differently and does not speak well enough. You should not indulge your child in everything and protect him from worries for fear of provoking an attack. In the future, any refusal will cause a reaction. If the baby is constantly at home, then it is better to think about visiting a preschool institution of any format. If respiratory attacks in children are a reaction to kindergarten, then it is worth taking a break from visits or changing the group.
The baby should not be overtired, thirsty or hungry. Fluctuations in blood glucose levels are also provocateurs of ARP. A negative aspect is often the excessive love of modern parents for developmental activities, when the child has to attend several early development schools at the same time.
You cannot deprive a child of his childhood!
It is necessary to provide full information to adults about the problem. Moms and dads must understand that the child’s seizures themselves are not dangerous and he will sooner or later outgrow them. However, you shouldn’t leave it to chance. Predisposition and hyperexcitability of the nervous system can develop into a more serious problem. Therefore, regular medical supervision is necessary.
Some tips to prevent new bouts of rolling
- Parents should be aware of the child’s condition. After all, everyone knows that a child is more likely to cry if he is hungry or tired, as well as in a situation where he cannot cope with any task. Try to mitigate or bypass all the causes of breath holding and convulsions: for example, if your baby gets irritated while rushing to get ready for a nursery or kindergarten, you better get up earlier to do it leisurely and measuredly.
- Be aware of how children perceive prohibitions. Try to use the word “cannot” as little as possible. But this in no way means that from now on everything is allowed for the baby! Just change the vector of its action. The baby will be more willing to comply with the suggestion: “Let’s go there!” than the requirement to stop immediately.
- Explain to your child what is happening to him. Say, “I know you’re angry because you didn’t get that toy.” And then make it clear that, despite his grief, there are limits to the expression of feelings: “You’re upset, but you shouldn’t yell in the store.”
- Explain the consequences of such actions: “If you yourself do not know how to stop in time, we will have to send you to your room.”
Clear boundaries of what is permitted, as well as a calm environment in the family, will help the child quickly cope with the feeling of panic and confusion that caused the rolling up.
Remember that any therapy in the case of affective-respiratory syndrome can only be prescribed by a neurologist, who will individually select the dose of the drug. Self-medication, as you probably understand, can be dangerous to your baby's health.
If you are faced with the problem of holding your breath in children, do not panic, since the child always comes out of this state on his own, without consequences, and gradually “outgrows” the described paroxysms.
Like all human diseases, ARP is easier to prevent than to treat, so once again I would like to remind you of the need for parents to have a flexible attitude towards the emotions of their child. Try to avoid situations that cause tantrums, and at the moment when the child is already on edge, postpone educational activities until a calmer time.
Remember: the child is not able to cope with this type of hysteria on his own, he cannot stop, and this, by the way, frightens him very much. Help him break this vicious circle.
Talk to him, don’t shout, show maximum patience and love, distract him, switch his attention to something pleasant, but do not give in to the baby’s obvious attempts to control you with attacks. If you grasp this line, then you most likely will not need drug treatment! Good luck and health!
Most often, such attacks should be expected in children who are easily excitable and irritable, they are capricious and overly vulnerable. Such symptoms can be classified as a type of early hysterical seizures. But for ordinary hysteria at an early age, specific primitive protest motor reactions are typical.
Children, if adults do not want to fulfill their wishes, in order to achieve their goals, fall to the floor and randomly flail their arms and legs on it, scream and sob heart-rendingly, in every possible way showing a storm of indignation and rage. The picture is familiar to many parents of three-year-olds. In such an emotional storm of protest behavior, features of the child’s later hysterical attacks can then be seen.
Of course, if the baby just falls to the floor and fights in hysterics, this will not surprise or pity the parents, but if breathing suddenly stops (although they do this unconsciously), then the effect is more impressive. After four years, such hysterics are less typical; they can continue or transform into other character problems. This can often be called crisis periods - three-year-olds, seven-year-olds, and then teenagers. Everything is rooted in childhood.
If you are faced with the problem of holding your breath in children, do not panic, since the child always comes out of this state on his own, without consequences, and gradually “outgrows” the described paroxysms.
Types of paroxysms and their characteristic symptoms
Affective-respiratory paroxysms can manifest themselves in different ways. Based on this, they are classified into types.
Depending on the clinical picture and the nature of the spasm of the respiratory muscles, the following types of breath-holding attacks in children are distinguished:
- complicated by ARP. Manifested by severe hypoxia of the brain. Holding your breath lasts longer than a minute. The child experiences involuntary urination, cramps in the arms and legs;
- simple ARP. Characterized by short-term breath holding. The attack lasts no more than 20 seconds. There are no signs of hypoxia and hypercapnia;
- white ARP. Manifested by shortness of breath and fainting. It develops quite quickly. The baby's skin in the chest, neck and face turns pale;
- blue ARP. The attack begins with hysterics. The child takes a sharp and deep breath, then holds his breath. Hyperemia of the epidermal covers is replaced by their cyanosis. Muscle tone decreases, the baby becomes weak. Possible loss of consciousness.
With a simple type of ARP, breathing is restored on its own. If the course is complicated, medical attention may be required. The clinical picture of affective-respiratory paroxysms is similar to the manifestations of epilepsy.
Therefore, it is necessary to conduct a full differential examination. The doctor may prescribe a blood test, ultrasound, ECG, EEG. The diagnosis of ARP is made if no organic disorders are identified.
Accepted classification
By the way, by the appearance of the face of a child who has had a seizure, you can determine the type of seizure. They are divided into:
- pale;
- blue.
Pale attacks occur in the event of a sudden fall or a strong blow to the baby. An injection can also lead to this condition. At such moments, the baby’s pulse cannot be felt, and he does not even have time to cry.
The causes of “blue” attacks lie in the child’s very strong resentment for something, disagreement with something, or uncontrollable rage. Such attacks occur most often in children aged 1.5-2.5 years. The child begins to be very capricious, cry, scream if something did not go the way he wanted it. At the moment of a very strong sigh in an involuntary manner, his breath will be held, and his face will acquire a bluish tint. Due to this situation, many children experience hypertonicity or a sharp decrease in muscle tone, as a result of which their body seems to go limp. The baby may arch. Although the situation is frightening, mostly children get out of it without the help of adults.
Causes
The main reasons may be refusal to fulfill his whim, if he does not get what he wants, or if he is simply not paid attention to when he wants it - the child begins to scream and cry. Deep breathing is interrupted from time to time, stopping on inspiration, the child becomes slightly cyanotic. In the best case, breathing will continue after a couple of seconds and the child will feel normal again. Externally, a “blue” attack is similar to a spasm of the muscles of the larynx, known as “laryngospasm”. In a more unfavorable case, it takes longer to manifest itself, as a result of which the child’s muscle tone decreases - in this case, he seems to “melt” in the mother’s arms; or vice versa - the muscles become very tense, causing it to arch. Most often they occur in hot-tempered, emotional and irritable children. They manifest themselves as hysterical attacks. A standard child's hysteria takes the form of protesting gestures - hitting the floor with their legs and arms, screaming, crying, showing dissatisfaction and rage.
From 3-4 years of age, a child with hysterical reactions or attacks of holding his breath differs from healthy children in his hysterics or problematic character. But there are ways to raise such children to prevent them from further developing a hysterical character as they grow up.
The basic principles of raising children with hysterical and respiratory-affective attacks are to prevent these attacks and educate the child to be restrained and control their emotions. Naturally, a surge of emotions is typical for all children and even adults. Adults, of course, know how to restrain their discontent. Children, for example, at the age of two are more open in this regard, since they have not yet been raised.